It is very easy to fill out the ncci nj erm 14 form. Our software was developed to be let you prepare any document easily. These are the four actions to go through:
Step 1: Find the button "Get Form Here" on the following site and click it.
Step 2: Now, you're on the file editing page. You may add content, edit present details, highlight particular words or phrases, insert crosses or checks, insert images, sign the file, erase unrequired fields, etc.
These particular sections will create the PDF form that you'll be filling in:
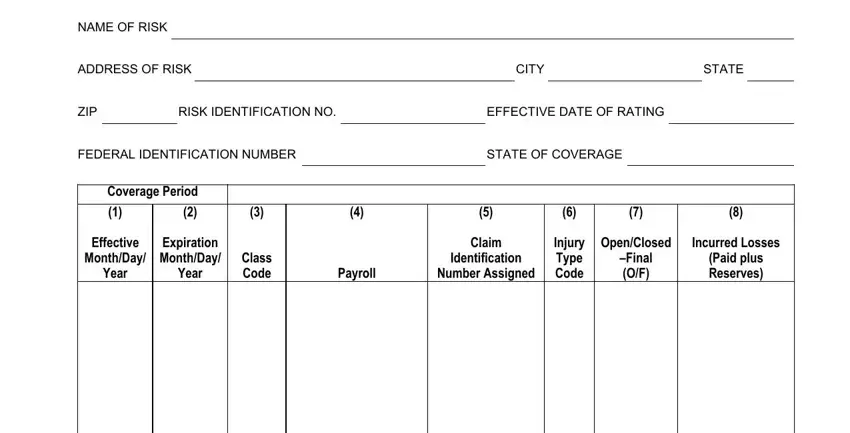
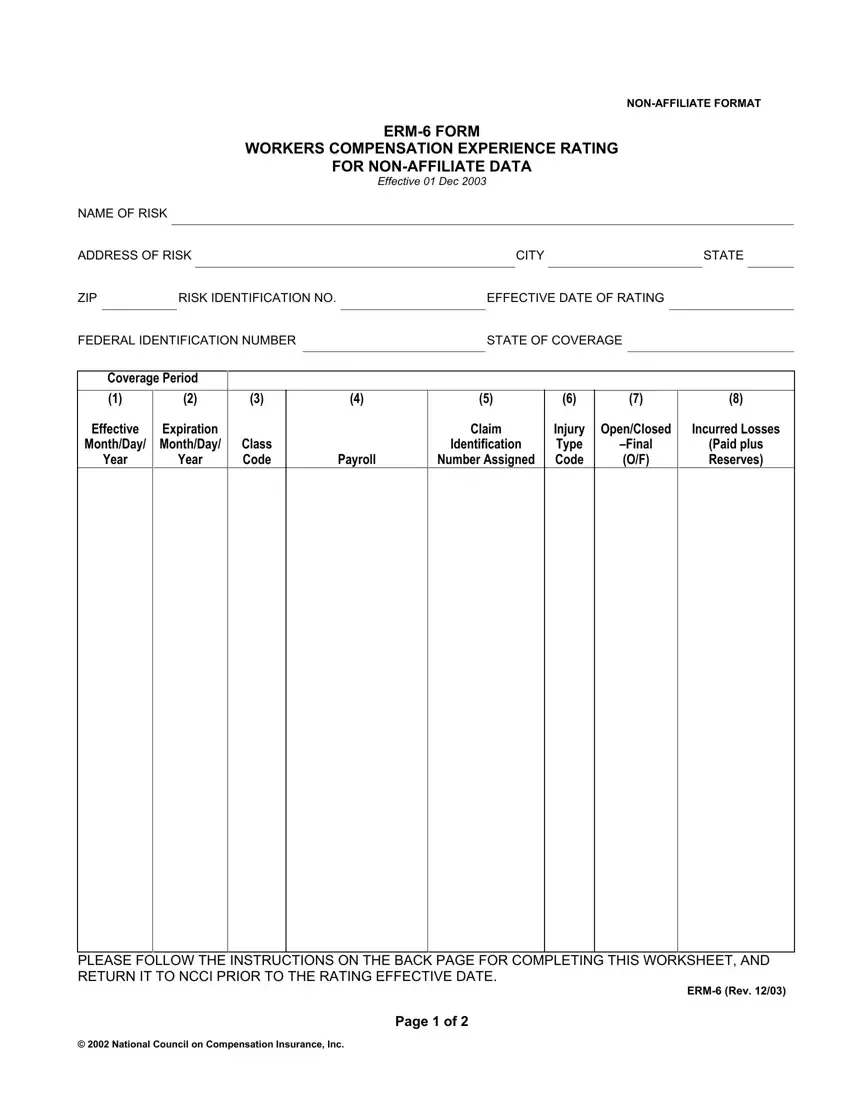
Fill in the PLEASE FOLLOW THE INSTRUCTIONS ON, ERM Rev, National Council on Compensation, and Page of fields with any details that are required by the application.
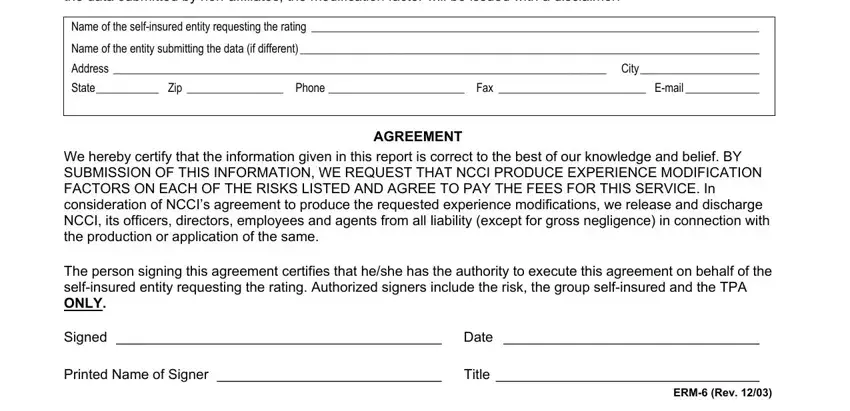
Point out the considerable details about the The experience rating will be, Name of the selfinsured entity, Name of the entity submitting the, Address City, State Zip Phone Fax Email, AGREEMENT, We hereby certify that the, The person signing this agreement, Signed Date, and Printed Name of Signer Title ERM box.
Step 3: Press "Done". Now you may transfer the PDF file.
Step 4: In order to prevent any type of risks later on, you should prepare at the very least several duplicates of the document.
