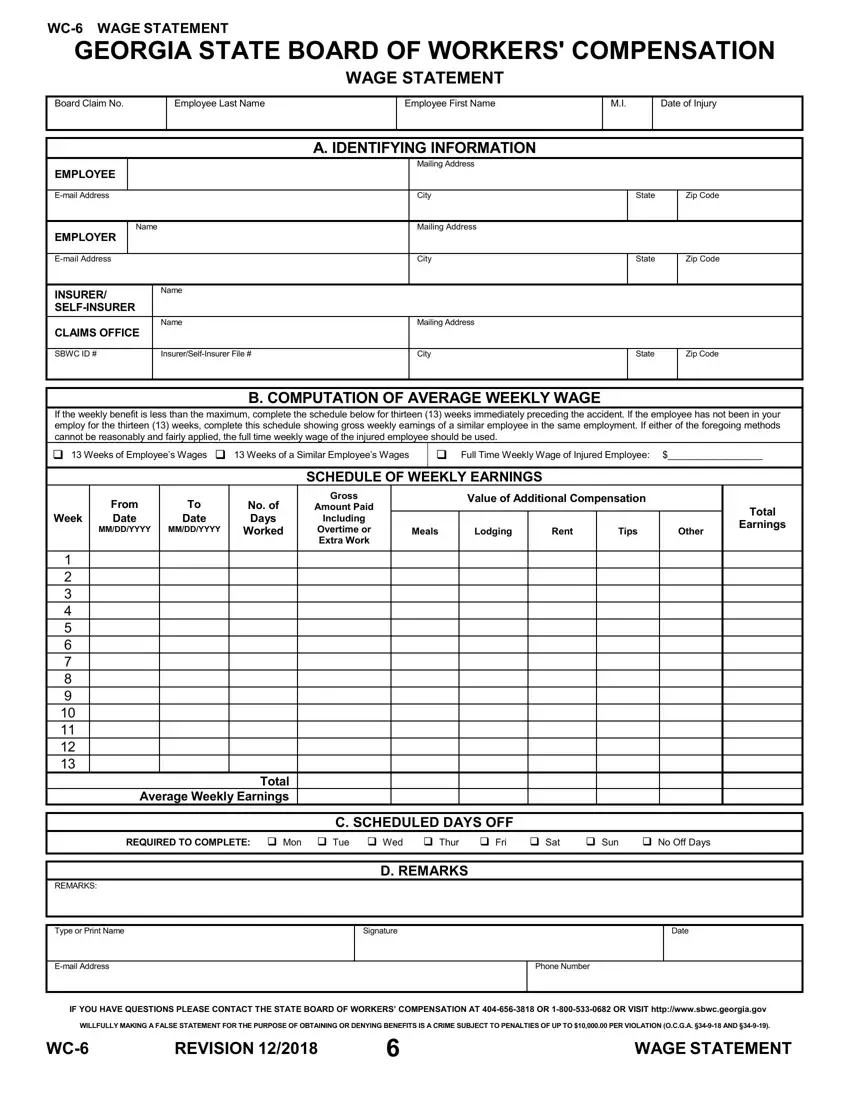
The Ga WC 6 form serves a critical role within the Georgia State Board of Workers' Compensation framework, providing a structured means for calculating an injured employee's average weekly wage. This document facilitates a fair assessment of benefits by requiring detailed wage information from both the employer and a comparable role within the same employment, should the employee not have a sufficient employment history. Key sections include identifying information for the employee, employer, and insurer or self-insurer, in addition to a comprehensive schedule for recording thirteen weeks of gross earnings leading up to the incident. This form not only assists in determining the financial compensation due to the employee but also underscores the state's commitment to protecting workers' rights through meticulous record-keeping and transparency. Instructions for completion are straightforward, with emphasis on the accuracy and honesty of the information provided, underlining the serious legal implications of falsifying documents. This wage statement is an invaluable tool, ensuring that workers are compensated in alignment with their earnings, thereby providing a semblance of security during their recovery period.
| Question | Answer |
|---|---|
| Form Name | Ga Form Wc 6 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 186 |
| Avg. time to fill out | 37 min 27 sec |
| Other names | georgia wage statement, wage state statement online, wc6, ga form wc |
