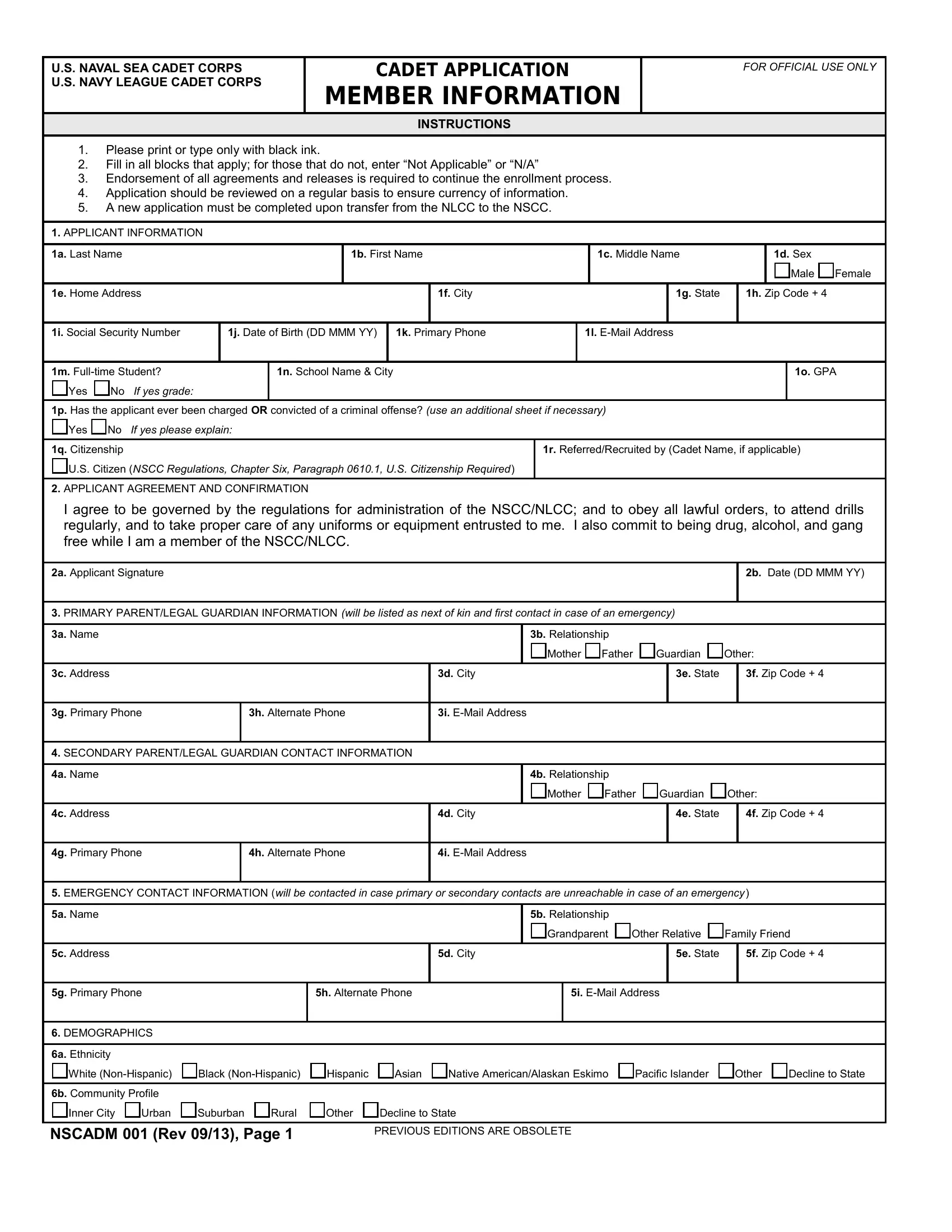
Embarking on a journey with the United States Naval Sea Cadet Corps (USNSCC) and the U.S. Navy League Cadet Corps requires the comprehensive completion of the NSCADM 001 form, a pivotal document designed to facilitate the enrollment process of prospective cadets. This form meticulously collects essential member information, ranging from basic identification details to detailed medical history, to ensure candidates are both prepared and eligible for the physical demands and structured discipline of cadet life. Applicants are advised to fill out the form with black ink, ensuring all relevant sections are accurately completed, and that any non-applicable fields are marked as such to avoid any processing delays. Moreover, the form calls for an agreement to abide by the corps' regulations and a commitment to maintaining a drug, alcohol, and gang-free lifestyle. The NSCADM 001 form not only serves as a gateway for young individuals aspiring to immerse themselves in military-aligned training but also involves a parental or guardian acknowledgment and consent section, emphasizing the shared responsibility and understanding required for the cadet's journey ahead. This detailed document, updated in its most recent revision, underlines the importance of accuracy and currency of information, reflecting the corps' commitment to the well-being, safety, and development of its members.
| Question | Answer |
|---|---|
| Form Name | Form Nscadm 001 |
| Form Length | 11 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 45 sec |
| Other names | Cadet_App_Membe r_Info nscadm001 form |