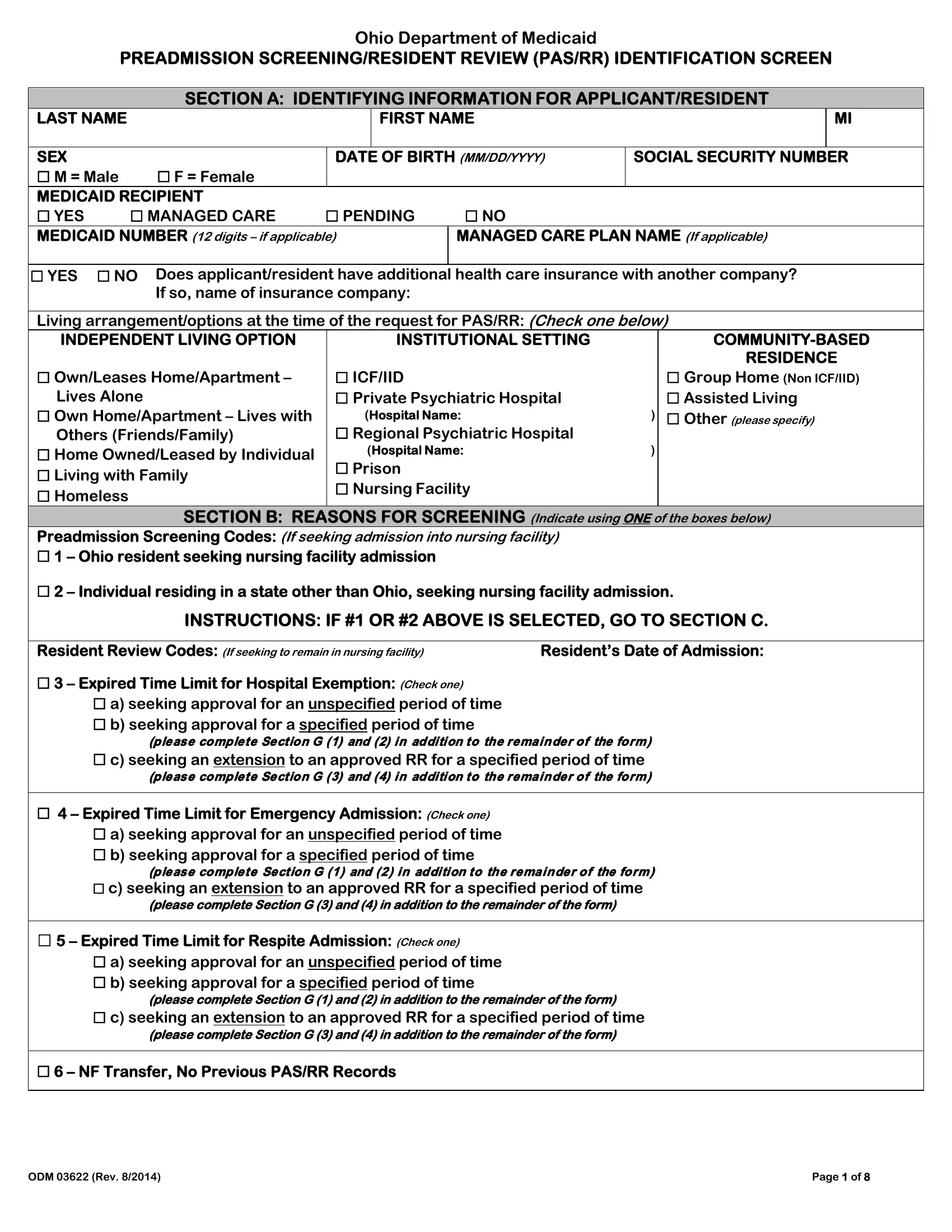
Understanding the complexities of the Medicaid system can be quite challenging, especially when it involves monitoring the care and services provided to individuals with specific health needs. The Ohio Department of Medicaid's ODM 03622 form, which is pertinent to the Preadmission Screening and Resident Review (PAS/RR), plays a crucial role in this process. This document is meticulously designed to ensure that individuals seeking admission into a nursing facility or those who are already residents receive the appropriate level of care, especially when mental illness or developmental disabilities are involved. By gathering comprehensive information on an applicant's medical diagnosis, indications of serious mental illness, and possible developmental disabilities or related conditions, the form guides the decision-making process. It aims to determine the most fitting living arrangement for the applicant, whether it be in an independent setting, a community-based option, or within an institutional environment. Additionally, the form touches on the significance of planning for a possible return to community living, emphasizing the importance of evaluating the individual's needs, aspirations, and the potential challenges they might face in such a transition. Through its detailed sections, the ODM 03622 form highlights the necessity of thorough assessment and ongoing review, ensuring that every individual's care journey is as informed and personalized as possible.
| Question | Answer |
|---|---|
| Form Name | Form Odm 03622 |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | oh pas rr, pasrr form ohio, 03622, ohio pas |