
You may work with miami dade certificate of occupancy without difficulty in our online tool for PDF editing. To have our tool on the leading edge of convenience, we work to integrate user-driven features and improvements on a regular basis. We're at all times happy to get feedback - play a pivotal role in revampimg how we work with PDF documents. Here's what you would have to do to get going:
Step 1: Hit the "Get Form" button in the top area of this page to access our PDF tool.
Step 2: The tool helps you change the majority of PDF files in many different ways. Change it with your own text, correct what's originally in the document, and include a signature - all within a couple of mouse clicks!
It is easy to complete the document with this detailed guide! Here is what you need to do:
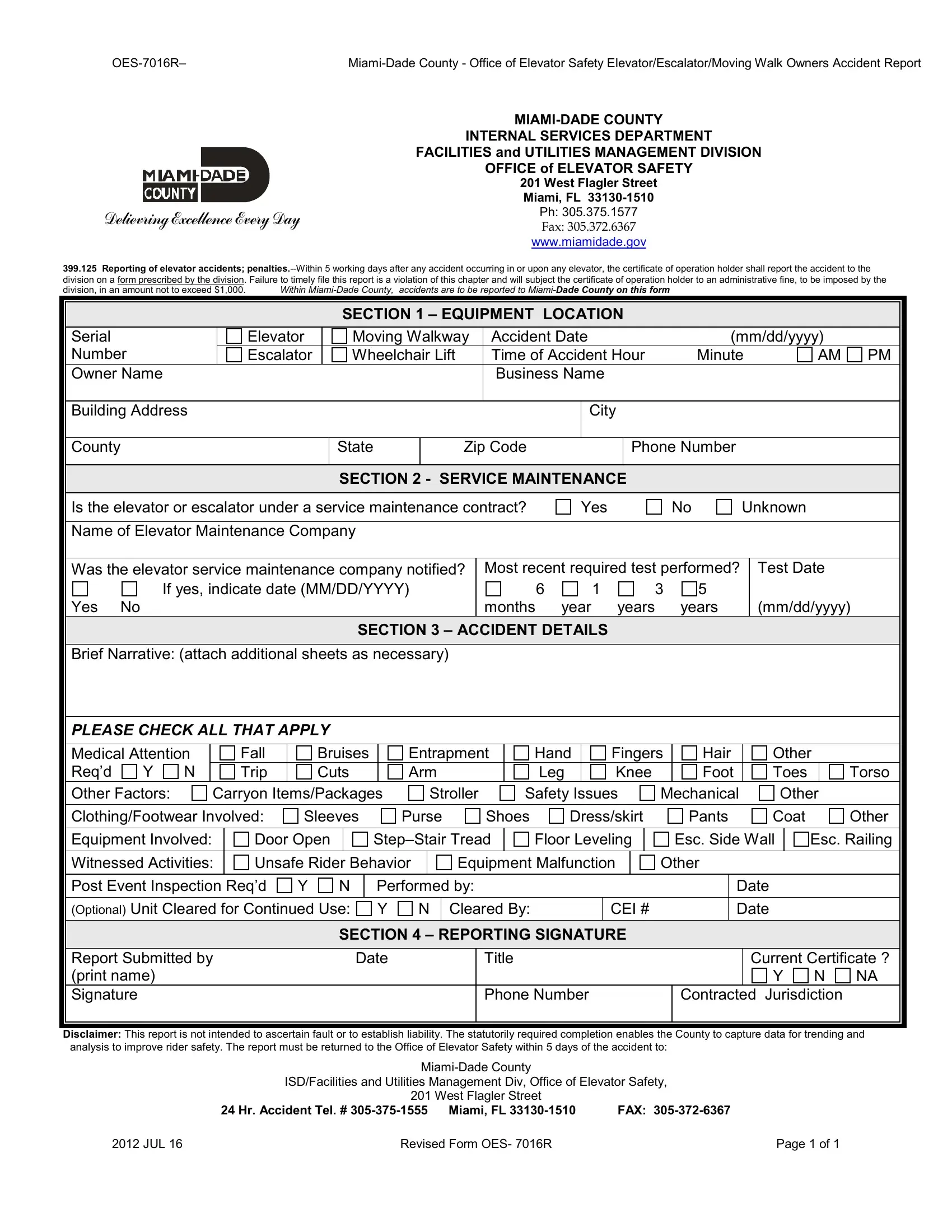
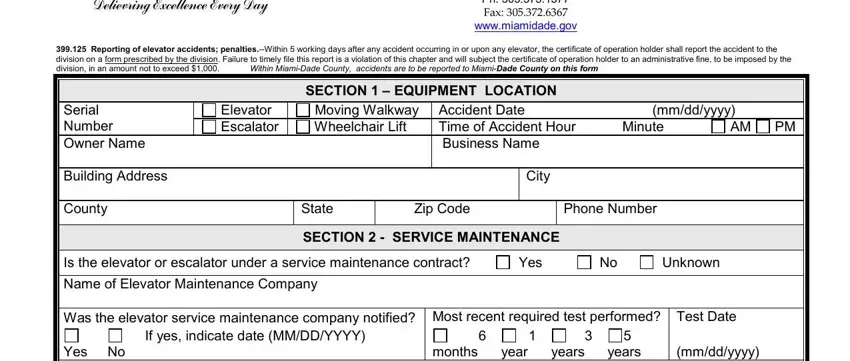
1. The miami dade certificate of occupancy necessitates certain information to be entered. Make sure the subsequent fields are completed:
2. The subsequent part is to fill out the next few blank fields: SECTION ACCIDENT DETAILS, Brief Narrative attach additional, Medical Attention N Reqd Other, Fall Trip, Bruises Cuts, Entrapment Arm, Hand Leg, Carryon ItemsPackages, Stroller, Safety Issues, Fingers Knee, Hair Foot Mechanical, Other Toes Other, Torso, and ClothingFootwear Involved.
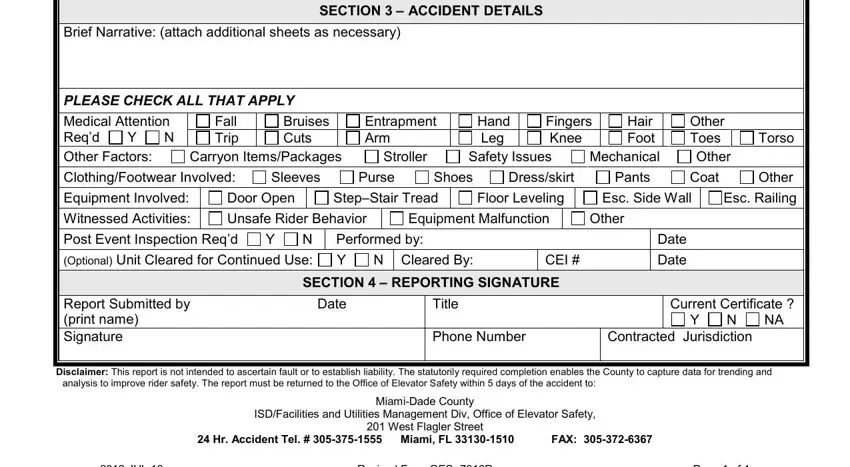
Be very attentive when filling out Fingers Knee and SECTION ACCIDENT DETAILS, since this is the part in which many people make a few mistakes.
Step 3: Check that your details are right and then simply click "Done" to conclude the project. After registering afree trial account at FormsPal, it will be possible to download miami dade certificate of occupancy or send it through email without delay. The document will also be readily available via your personal account menu with all of your edits. We do not share any information that you provide when filling out documents at our website.