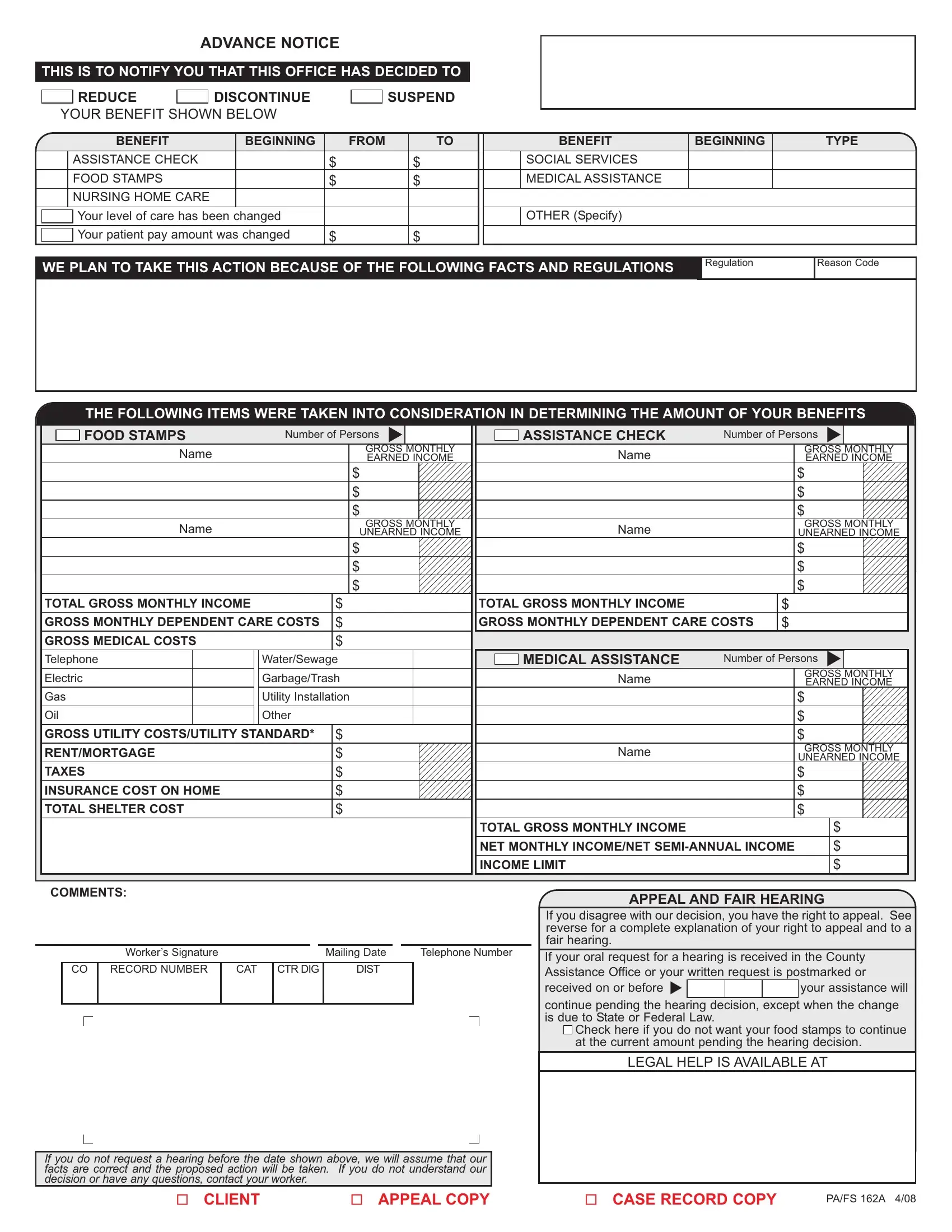
Navigating the complexities of benefit adjustments can be challenging for individuals relying on assistance programs. The Pa FS 162A form serves as a critical tool in this process, providing recipients with advance notice of any planned changes to their benefits, including discontinuation, reduction, or suspension. This form covers a range of programs such as assistance checks, social services, food stamps, medical assistance, and nursing home care, detailing the type and extent of changes alongside the specific starting dates. Moreover, it outlines the reason for these adjustments, referencing the relevant regulations and reason codes. Recipients are informed about the considerations taken into account when determining their benefit amounts, including household composition, income, dependent care costs, and shelter expenses. Importantly, the document also explains the rights of recipients to appeal these decisions, offering a pathway to request a hearing and potentially contest the changes made to their benefits. This ensures individuals are not only aware of how their assistance might change but also understand their rights to challenge these decisions if they believe them to be incorrect or unjust.
| Question | Answer |
|---|---|
| Form Name | Form Pa Fs 162A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | pa fs 162 form, pa fs 162, fs pa 162, Washington |