
With the online PDF editor by FormsPal, you are able to fill out or edit Cephalosporins here. Our development team is continuously endeavoring to expand the tool and ensure it is much easier for people with its cutting-edge features. Bring your experience to another level with continually growing and great options available today! By taking several basic steps, you may begin your PDF journey:
Step 1: Click on the orange "Get Form" button above. It's going to open up our pdf editor so that you can start filling in your form.
Step 2: Using this online PDF tool, you'll be able to accomplish more than merely complete blank fields. Express yourself and make your documents seem high-quality with customized textual content put in, or optimize the original input to perfection - all backed up by the capability to add any type of images and sign it off.
Be mindful when completing this document. Make sure that every blank is filled in accurately.
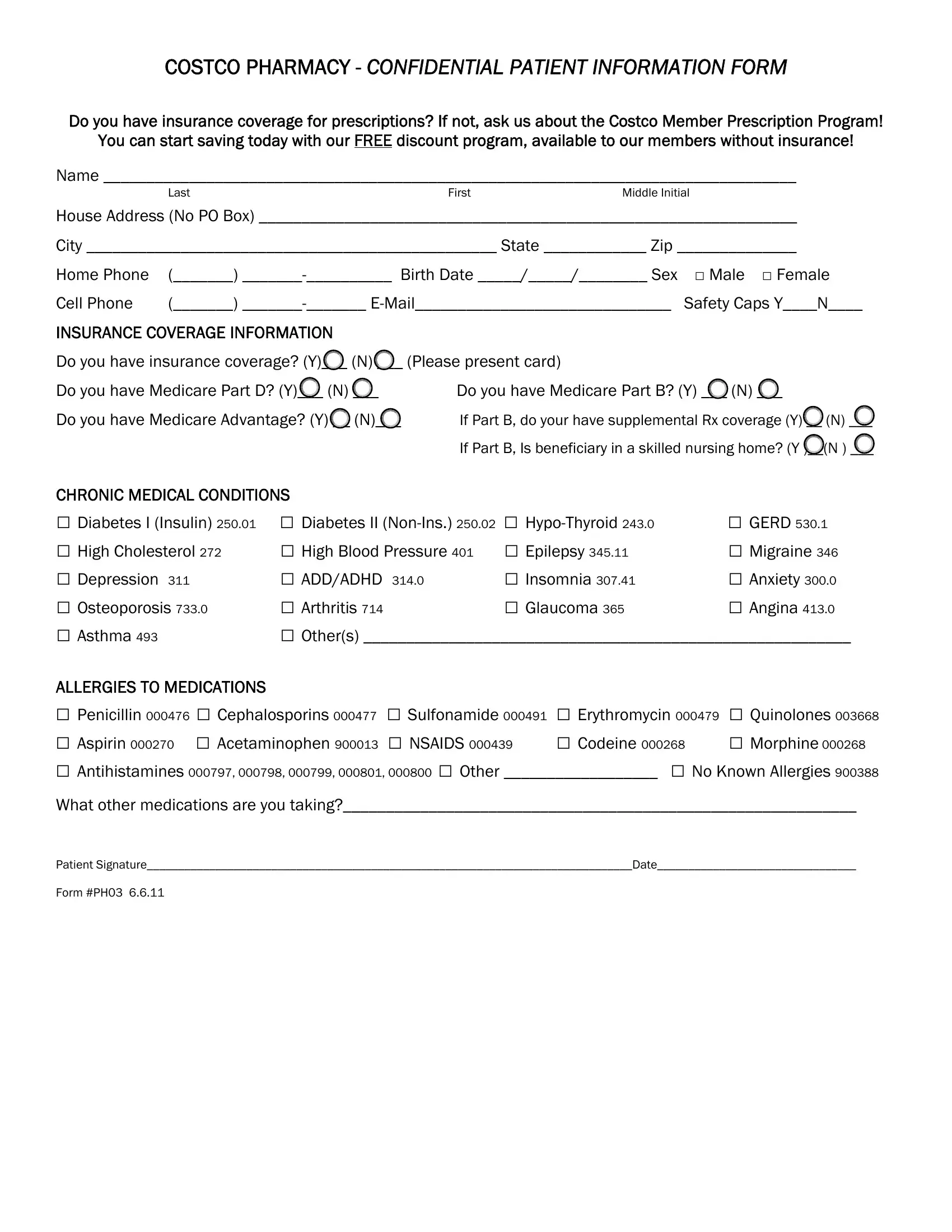
1. To start off, when filling out the Cephalosporins, start in the area with the following blanks:
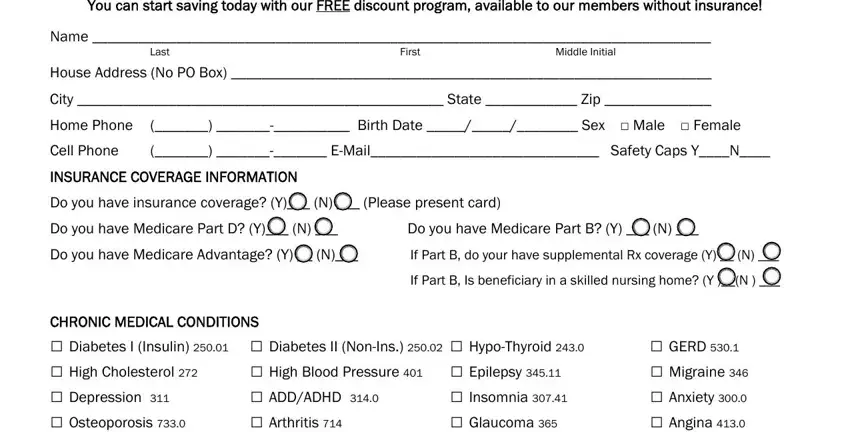
2. After filling out the previous part, go on to the subsequent stage and fill out the necessary particulars in these fields - Diabetes I Insulin Diabetes II, High Blood Pressure Epilepsy, GERD Migraine Anxiety, ALLERGIES TO MEDICATIONS, Penicillin Cephalosporins, and What other medications are you.
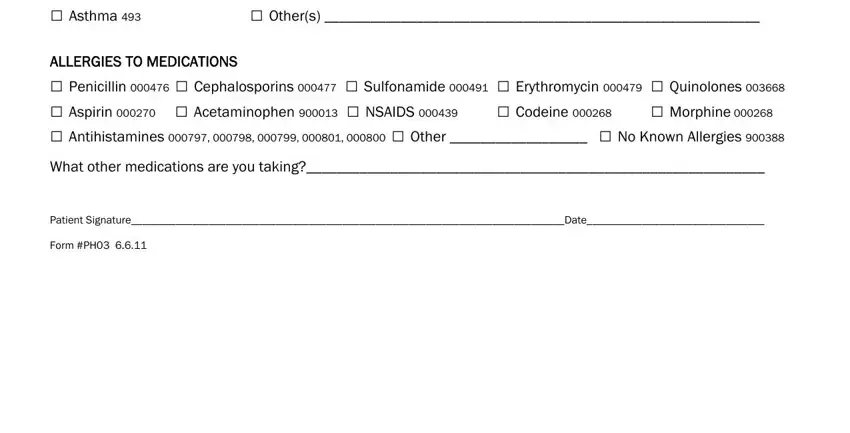
Always be really careful when filling out What other medications are you and ALLERGIES TO MEDICATIONS, since this is where many people make mistakes.
Step 3: Reread the details you've typed into the blank fields and then click on the "Done" button. Make a 7-day free trial plan at FormsPal and acquire instant access to Cephalosporins - downloadable, emailable, and editable in your personal account. When using FormsPal, you can easily complete forms without the need to get worried about personal data leaks or data entries getting shared. Our secure system makes sure that your personal information is stored safely.