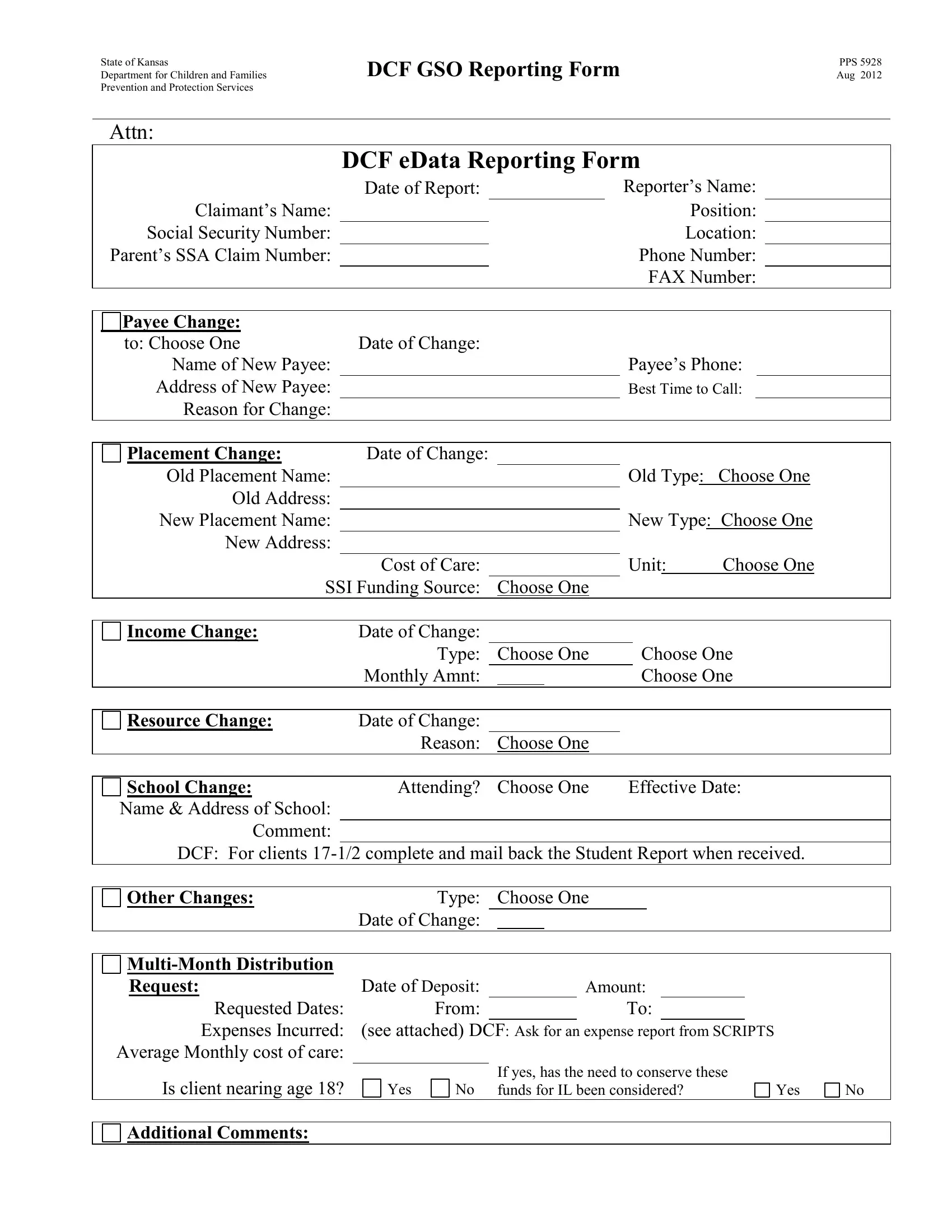
The State of Kansas Department for Children and Families (DCF) has developed a comprehensive form, PPS 5928, aimed at integrating various aspects of child welfare reporting. This form plays a crucial role in updating and maintaining the health and safety of children under the care of the Department, providing a structured way to report changes in the claimant's situation including but not limited to payee changes, placement adjustments, income variations, and schooling details. By meticulously capturing details such as the claimant's name, date of the report, reporter's name and position, and specifics about any changes such as the new payee's information or changes in the placement of a child, the form enables accurate tracking and timely interventions. Additionally, it addresses the financial aspects related to the care of the children, including expenses incurred, changes in cost of care, and adjustments in Social Security Income (SSI) funding sources, ensuring that the economic factors affecting the welfare of the children are promptly dealt with. With provisions to report on essential changes and requests, including those leading up to when a client nears age 18, the form also prompts considerations for the transition into independent living, making it an essential instrument for the structured and effective management of child welfare within the state.
| Question | Answer |
|---|---|
| Form Name | Form Pps 5928 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | student dcf bengali meaning, student dcf, dcf full form in bengali, dcf full form |
State of Kansas
Department for Children and FamiliesDCF GSO Reporting Form Prevention and Protection Services
Attn:
DCF eData Reporting Form
PPS 5928 Aug 2012
|
|
Claimant’s Name: |
|
Date of Report: |
|
|
|
|
|
|
Reporter’s Name: |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Position: |
|
|||||||
|
|
Social Security Number: |
|
|
|
|
|
|
|
|
|
|
|
Location: |
|
|||||
|
Parent’s SSA Claim Number: |
|
|
|
|
|
|
|
|
|
Phone Number: |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FAX Number: |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Payee Change: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
to: Choose One |
Date of Change: |
|
|
|
|
|
|
Payee’s Phone: |
|
|||||||||
|
|
Name of New Payee: |
|
|
|
|
|
|
|
|
||||||||||
|
|
Address of New Payee: |
|
|
|
|
|
|
|
|
Best Time to Call: |
|
||||||||
|
|
Reason for Change: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Placement Change: |
Date of Change: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Old Placement Name: |
|
|
|
|
|
|
|
|
Old Type: |
Choose One |
||||||||
|
|
Old Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
New Placement Name: |
|
|
|
|
|
|
|
|
New Type: Choose One |
|||||||||
|
|
New Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Cost of Care: |
|
|
|
|
|
|
Unit: |
Choose One |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
SSI Funding Source: Choose One |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Income Change: |
Date of Change: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Type: |
|
|
Choose One |
|
|
Choose One |
|||||||||
|
|
|
|
|
Monthly Amnt: |
|
|
|
|
|
|
|
Choose One |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Resource Change: |
Date of Change: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Reason: |
|
|
Choose One |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
School Change: |
Attending? |
|
|
Choose One |
|
Effective Date: |
||||||||||||
|
Name & Address of School: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Comment: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DCF: For clients |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Other Changes: |
Type: |
|
|
Choose One |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
Date of Change: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Request: |
Date of Deposit: |
|
|
|
|
Amount: |
|
|
|
|
|
|
||||||
|
|
Requested Dates: |
From: |
|
|
|
|
|
|
To: |
|
|
|
|
|
|
||||
Expenses Incurred: (see attached) DCF: Ask for an expense report from SCRIPTS Average Monthly cost of care:
Is client nearing age 18?
Yes
|
If yes, has the need to conserve these |
No |
funds for IL been considered? |
Yes
No
Additional Comments: