
You can work with HIPAA instantly with the help of our PDFinity® editor. The tool is consistently updated by our team, receiving powerful functions and growing to be a lot more versatile. To get started on your journey, go through these simple steps:
Step 1: Click on the "Get Form" button at the top of this page to open our PDF tool.
Step 2: With this online PDF file editor, you can actually accomplish more than simply fill in blank form fields. Express yourself and make your forms look perfect with customized textual content incorporated, or adjust the file's original content to perfection - all that comes along with an ability to insert your personal pictures and sign the PDF off.
It is actually straightforward to complete the document using this detailed tutorial! This is what you want to do:
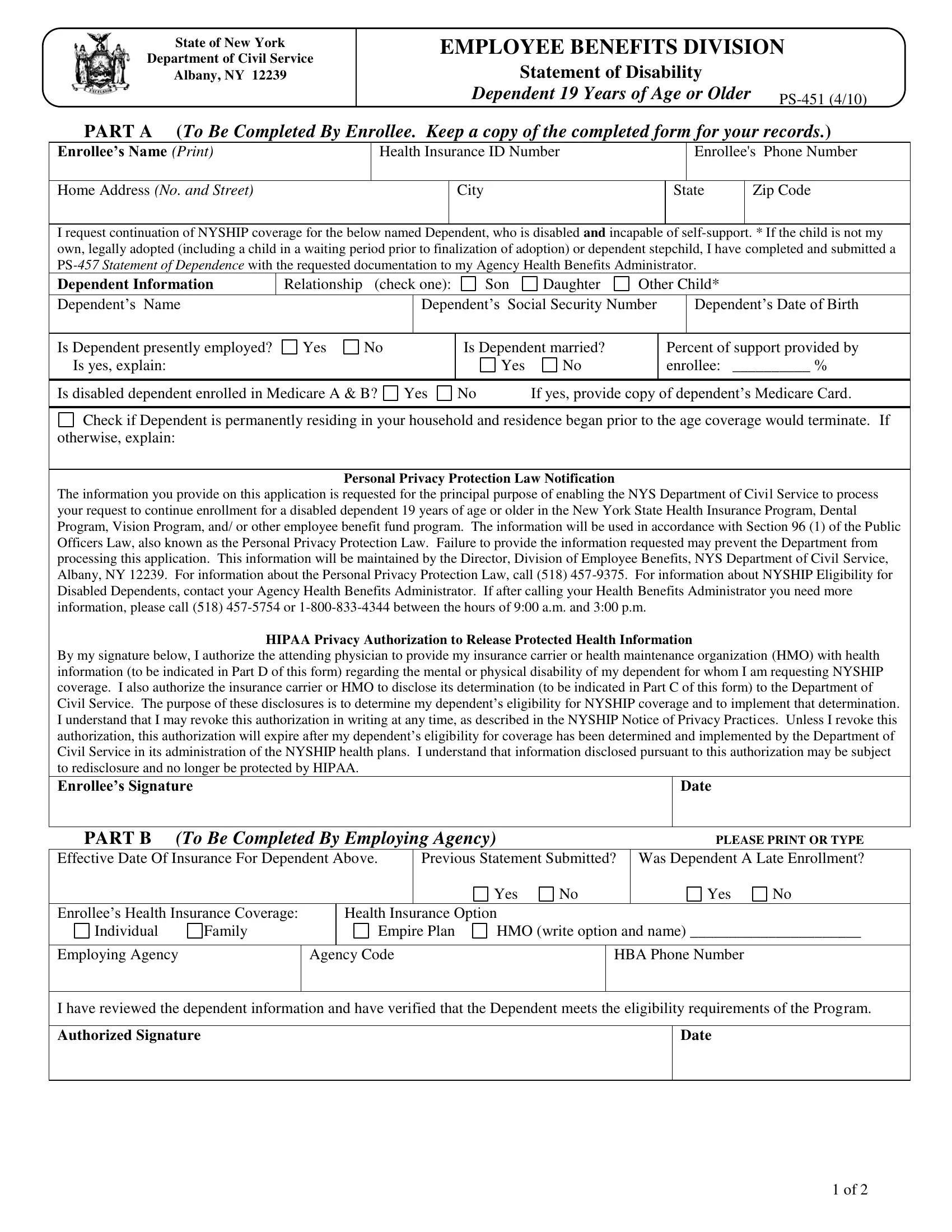
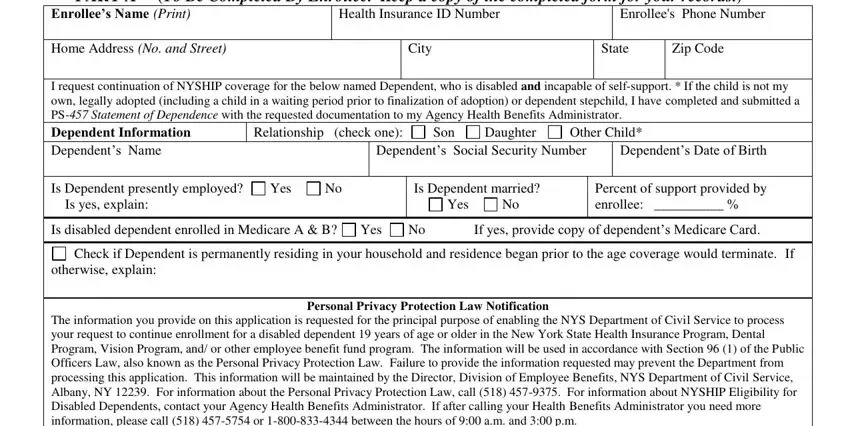
1. Begin completing your HIPAA with a selection of major blanks. Get all of the required information and make sure there's nothing forgotten!
2. Once your current task is complete, take the next step – fill out all of these fields - By my signature below I authorize, Date, Effective Date Of Insurance For, PART B To Be Completed By, Previous Statement Submitted, Yes, Yes, Enrollees Health Insurance Coverage, Individual, Family, Health Insurance Option, Empire Plan, HMO write option and name, Employing Agency, and Agency Code with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
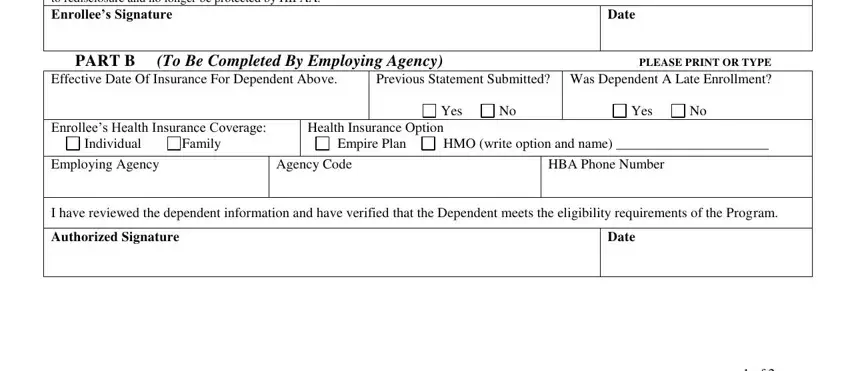
It's easy to get it wrong when filling in your HMO write option and name, consequently make sure you look again prior to when you finalize the form.
Step 3: Before finalizing your document, double-check that blank fields have been filled out properly. Once you believe it's all fine, press “Done." Grab your HIPAA after you register at FormsPal for a 7-day free trial. Quickly use the form within your personal cabinet, with any modifications and changes being all kept! Whenever you work with FormsPal, you can complete documents without needing to worry about data incidents or records getting shared. Our protected software ensures that your personal information is kept safely.