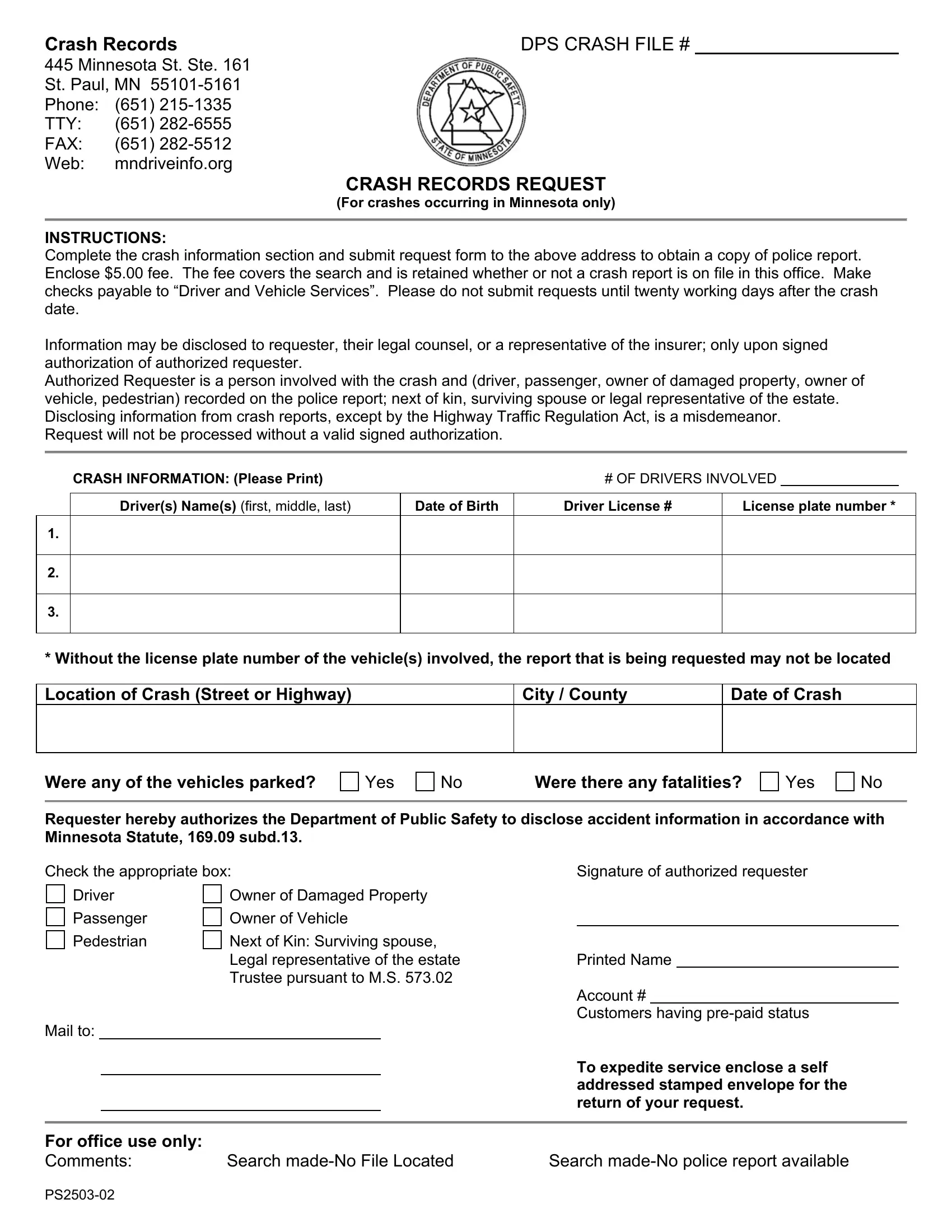
Understanding the intricacies of the PS2503-02 form is vital for anyone involved in a vehicle crash in Minnesota and seeking to obtain a crash report. This document serves as a formal request to the Department of Public Safety, specifically aimed at the Crash Records section located at 445 Minnesota Street, Ste. 161, St. Paul, MN. Those needing the crash information must fill out the form accurately, providing details such as the number of drivers involved, names, dates of birth, driver license numbers, license plate numbers, the crash location, city/county, date, and specifics about the crash, including fatalities or if any vehicles were parked. A fee of $5.00 is required with the submission, covering the search for the record, which is non-refundable even if the report is not found in the office's files. Payments should be made payable to “Driver and Vehicle Services”. Importantly, requests are advised to be made no less than twenty working days following the crash date to allow for processing and record availability. The form highlights who can request these records—ranging from directly involved parties, next of kin, to legal representatives—underscoring the legal stipulation that crash report information can only be disclosed under authorized conditions. In doing so, it also emphasizes the legal implications of unauthorized disclosure. This form plays a crucial role in ensuring that individuals or their representatives can access critical information for various purposes, including legal and insurance claims, while adhering to Minnesota's regulations on crash report dissemination.
| Question | Answer |
|---|---|
| Form Name | Form Ps2503 02 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | pre, Enclose, mn crash record request, Ste |
Crash Records |
DPS CRASH FILE # |
445 Minnesota St. Ste. 161 St. Paul, MN
CRASH RECORDS REQUEST
(For crashes occurring in Minnesota only)
INSTRUCTIONS:
Complete the crash information section and submit request form to the above address to obtain a copy of police report. Enclose $5.00 fee. The fee covers the search and is retained whether or not a crash report is on file in this office. Make checks payable to “Driver and Vehicle Services”. Please do not submit requests until twenty working days after the crash date.
Information may be disclosed to requester, their legal counsel, or a representative of the insurer; only upon signed authorization of authorized requester.
Authorized Requester is a person involved with the crash and (driver, passenger, owner of damaged property, owner of vehicle, pedestrian) recorded on the police report; next of kin, surviving spouse or legal representative of the estate. Disclosing information from crash reports, except by the Highway Traffic Regulation Act, is a misdemeanor.
Request will not be processed without a valid signed authorization.
CRASH INFORMATION: (Please Print) |
|
# OF DRIVERS INVOLVED |
|
|
|
|
|
|
|
|
|
Driver(s) Name(s) (first, middle, last) |
Date of Birth |
Driver License # |
License plate number * |
|
|
1.
2.
3.
* Without the license plate number of the vehicle(s) involved, the report that is being requested may not be located
Location of Crash (Street or Highway)
City / County
Date of Crash
Were any of the vehicles parked?
Yes
No |
Were there any fatalities? |
Yes
No
Requester hereby authorizes the Department of Public Safety to disclose accident information in accordance with Minnesota Statute, 169.09 subd.13.
Check the appropriate box:
Driver |
Owner of Damaged Property |
|||
Passenger |
Owner of Vehicle |
|||
Pedestrian |
Next of Kin: Surviving spouse, |
|||
|
|
|
Legal representative of the estate |
|
|
|
|
Trustee pursuant to M.S. 573.02 |
|
Mail to: |
|
|
||
|
|
|
|
|
|
|
|
|
|
Signature of authorized requester
Printed Name
Account #
Customers having
To expedite service enclose a self addressed stamped envelope for the return of your request.
For office use only: |
|
|
Comments: |
Search |
Search |