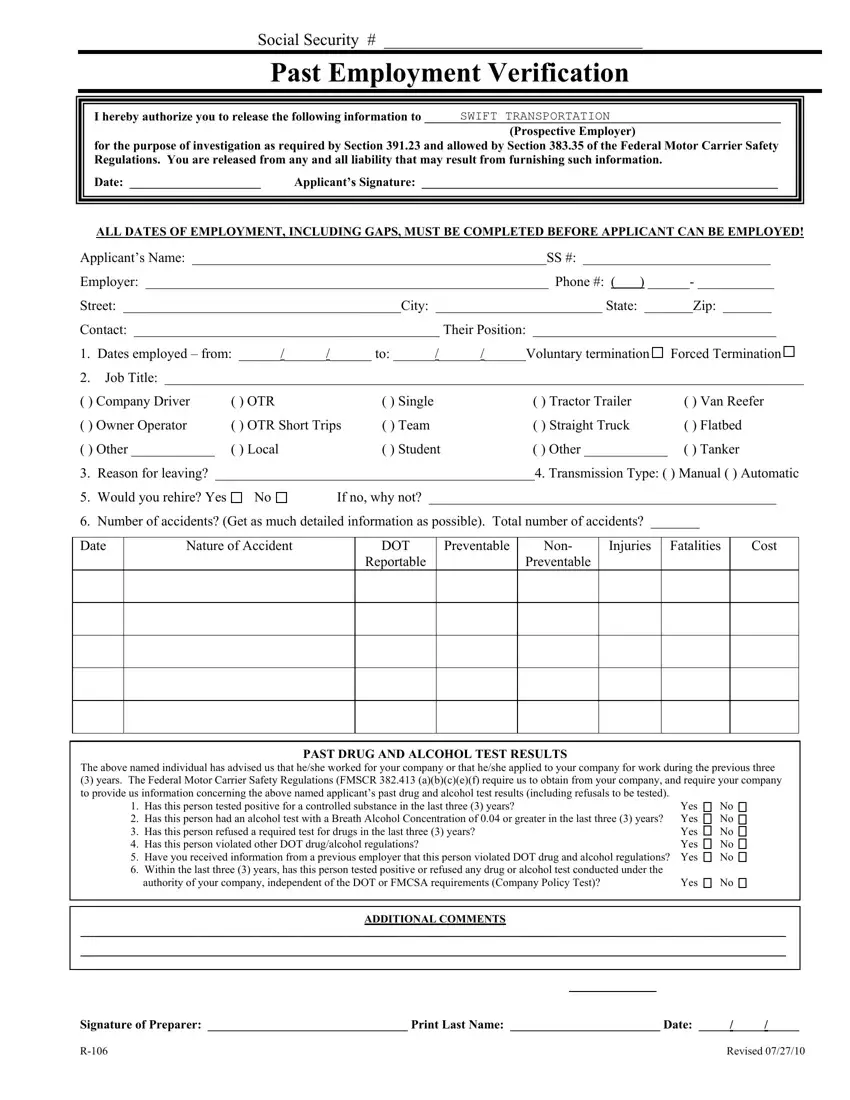
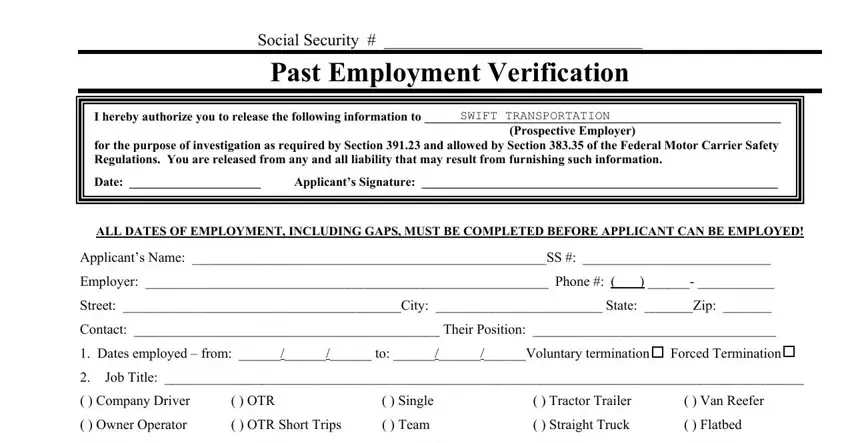
Social Security # _______________________________ |
Past Employment Verification |
I hereby authorize you to release the following information to |
SWIFT TRANSPORTATION |
(Prospective Employer)
for the purpose of investigation as required by Section 391.23 and allowed by Section 383.35 of the Federal Motor Carrier Safety Regulations. You are released from any and all liability that may result from furnishing such information.
Date: _____________________ |
Applicant’s Signature: _________________________________________________________ |
ALL DATES OF EMPLOYMENT, INCLUDING GAPS, MUST BE COMPLETED BEFORE APPLICANT CAN BE EMPLOYED!
Applicant’s Name: ___________________________________________________SS #: ___________________________
Employer: __________________________________________________________ Phone #: ( ) ______- ___________
Street: ________________________________________City: ________________________ State: _______Zip: _______
Contact: ____________________________________________ Their Position: ___________________________________
1.Dates employed – from: ______/______/______ to: ______/______/______Voluntary termination 
 Forced Termination
Forced Termination 

2.Job Title: ____________________________________________________________________________________________
( ) Company Driver |
( ) OTR |
( ) Single |
( ) Tractor Trailer |
( ) Van Reefer |
( ) Owner Operator |
( ) OTR Short Trips |
( ) Team |
( ) Straight Truck |
( ) Flatbed |
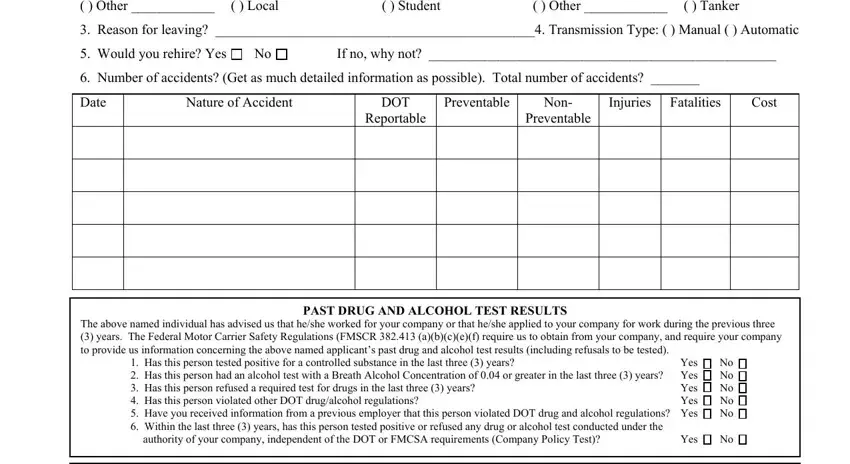
( ) Other ____________ |
( ) Local |
( ) Student |
( ) Other ____________ |
( ) Tanker |
3. |
Reason for leaving? ______________________________________________4. Transmission Type: ( ) Manual ( ) Automatic |
5. Would you rehire? Yes |
No |
If no, why not? __________________________________________________ |
6. Number of accidents? (Get as much detailed information as possible). Total number of accidents? _______ |
|
|
|
|
|
|
|
|
|
|
Date |
Nature of Accident |
|
DOT |
Preventable |
Non- |
Injuries |
Fatalities |
Cost |
|
|
|
|
|
Reportable |
|
Preventable |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAST DRUG AND ALCOHOL TEST RESULTS
The above named individual has advised us that he/she worked for your company or that he/she applied to your company for work during the previous three
(3)years. The Federal Motor Carrier Safety Regulations (FMSCR 382.413 (a)(b)(c)(e)(f) require us to obtain from your company, and require your company to provide us information concerning the above named applicant’s past drug and alcohol test results (including refusals to be tested).
1. |
Has this person tested positive for a controlled substance in the last three (3) years? |
Yes |
|
No |
2. |
Has this person had an alcohol test with a Breath Alcohol Concentration of 0.04 or greater in the last three (3) years? |
Yes |
|
No |
|
3. |
Has this person refused a required test for drugs in the last three (3) years? |
Yes |
|
No |
|
|
4. |
Has this person violated other DOT drug/alcohol regulations? |
Yes |
|
No |
|
5.Have you received information from a previous employer that this person violated DOT drug and alcohol regulations? Yes 
 No
No 

6.Within the last three (3) years, has this person tested positive or refused any drug or alcohol test conducted under the
authority of your company, independent of the DOT or FMCSA requirements (Company Policy Test)? |
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDITIONAL COMMENTS |
|
|
|
|
|
_______________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________
Signature of Preparer: ________________________________ Print Last Name: ________________________ Date: _____/_____/_____