
nys wcb rb 89 1 can be filled out online effortlessly. Just use FormsPal PDF tool to complete the task right away. In order to make our editor better and easier to utilize, we constantly develop new features, with our users' feedback in mind. Getting underway is easy! Everything you need to do is follow the next simple steps below:
Step 1: Hit the orange "Get Form" button above. It's going to open up our editor so you could start filling out your form.
Step 2: This tool helps you customize PDF forms in a variety of ways. Change it with your own text, correct what is already in the document, and add a signature - all within several mouse clicks!
This form will need particular details to be typed in, so you must take the time to type in what's asked:
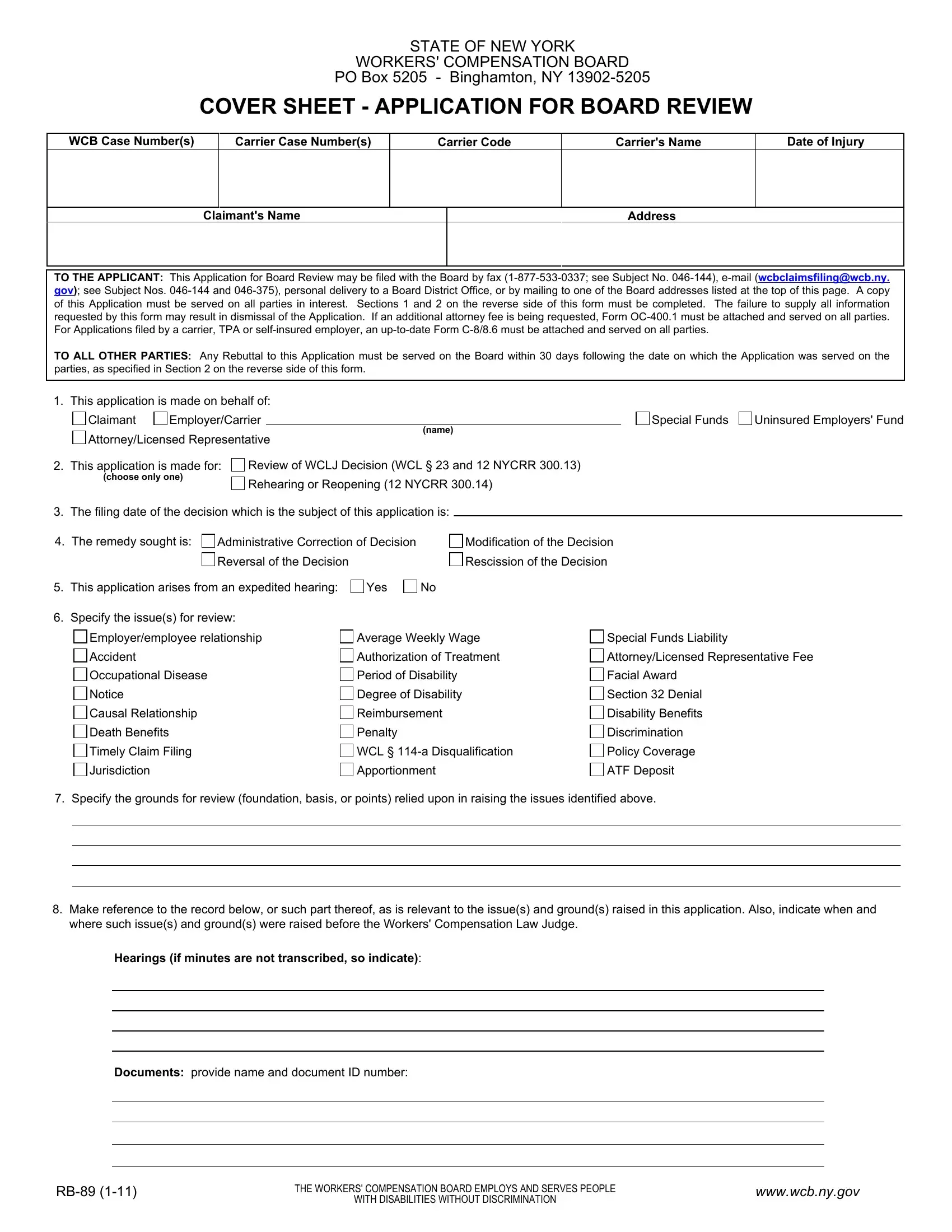
1. The nys wcb rb 89 1 involves particular information to be entered. Ensure the following fields are finalized:
2. After the last array of fields is complete, you should put in the required specifics in This application arises from an, Specify the issues for review, Employeremployee relationship, Average Weekly Wage, Special Funds Liability, Accident, Occupational Disease, Notice, Causal Relationship, Death Benefits, Timely Claim Filing, Jurisdiction, Authorization of Treatment, AttorneyLicensed Representative Fee, and Period of Disability so you can progress further.
Be very attentive when filling in Accident and Authorization of Treatment, since this is where a lot of people make a few mistakes.
3. Throughout this stage, look at Documents provide name and, THE WORKERS COMPENSATION BOARD, WITH DISABILITIES WITHOUT, and wwwwcbnygov. Each one of these should be taken care of with utmost precision.

4. All set to fill in the next part! In this case you've got all these Transcripts provide date and, NonScanable Evidence or Videotape, List the following periods andor, A Form OC for an increased, Yes, Certification By signing this, Signature of Person Preparing Form, Date, Print Name, Title, and Phone Number empty form fields to do.

5. To conclude your document, this final part incorporates a couple of extra blank fields. Completing Address, and SECTION AFFIRMATION STATE OF NEW should wrap up everything and you will be done very fast!
Step 3: Ensure that the details are correct and click on "Done" to conclude the task. Right after creating a7-day free trial account at FormsPal, you'll be able to download nys wcb rb 89 1 or send it via email right off. The form will also be available from your personal cabinet with all of your changes. FormsPal guarantees your data privacy with a secure system that in no way records or distributes any sensitive information used in the PDF. Be confident knowing your docs are kept confidential each time you use our services!