Form Sf 6 is the standard form for submission of Unclassified Controlled Information to DoD components. The form allows for submission of information by those with a need to know and provides for a method to track the receipt, review and declassification of the submitted information. By using Form Sf 6, submitters can ensure that their information is handled in a controlled and consistent manner. The use of Form Sf 6 is mandatory for all unclassified controlled information submissions. Failure to use Form Sf 6 may result in delays or rejection of your submission. For more information on how to complete and submit Form Sf 6, please visit our website. Thank you for your cooperation!
| Question | Answer |
|---|---|
| Form Name | Form Sf 6 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | AWCC, ARKANSAS, Claimant, fwisd affidavit of residency |
Form
Rev.
Autho rity:
Ark. Code Ann.
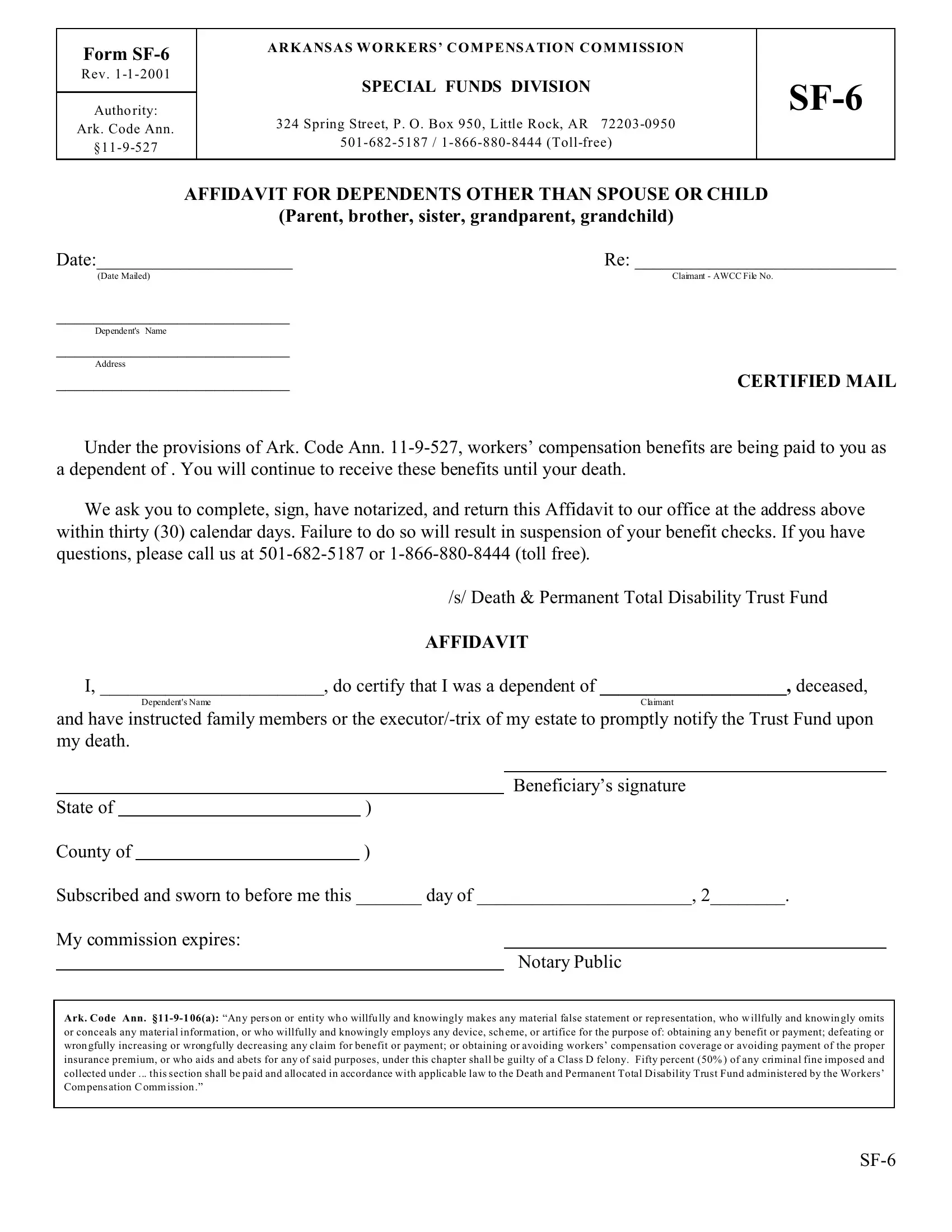
A R K A NS A S W O R K E RS ’ C O M P E NS A TIO N C O M M I SS IO N
SPECIAL FUNDS DIVISION
324 Spring Street, P. O. Box 950, Little Rock, AR
AFFIDAVIT FOR DEPENDENTS OTHER THAN SPOUSE OR CHILD
(Parent, brother, sister, grandparent, grandchild)
Date:_____________________ |
Re: ____________________________ |
(Date Mailed) |
Claimant - AWCC File No. |
_________________________ |
|
Dependent's Name |
|
_________________________ |
|
Address |
|
_________________________ |
CERTIFIED MAIL |
Under the provisions of Ark. Code Ann.
We ask you to complete, sign, have notarized, and return this Affidavit to our office at the address above within thirty (30) calendar days. Failure to do so will result in suspension of your benefit checks. If you have questions, please call us at
/s/ Death & Permanent Total Disability Trust Fund
AFFIDAVIT
I, ________________________, do certify that I was a dependent of ____________________, deceased,
Dependent's Name |
Claimant |
and have instructed family members or the
|
|
|
|
Beneficiary’s signature |
State of |
|
) |
|
|
County of |
|
) |
|
|
Subscribed and sworn to before me this _______ day of _______________________, 2________.
My commission expires:
Notary Public
Ark. Code Ann.
or conceals any material information, or who willfully and knowingly employs any device, sch eme, or artifice for the purpose of: obtaining an y benefit or payment; defeating or wron gfully increasing or wrongfully decreasing any claim for benefit or payment; or obtaining or avoiding workers’ compensation coverage or avoiding payment of the proper insurance premium, or who aids and abets for any of said purposes, under this chapter shall be guilty of a Class D felony. Fifty percent (50% ) of any criminal fine imposed and collected under ... this section shall be paid and allocated in accordance with applicable law to the Death and Permanent Total Disability Trust Fund administered by the Workers’ Com pens ation C omm ission .”