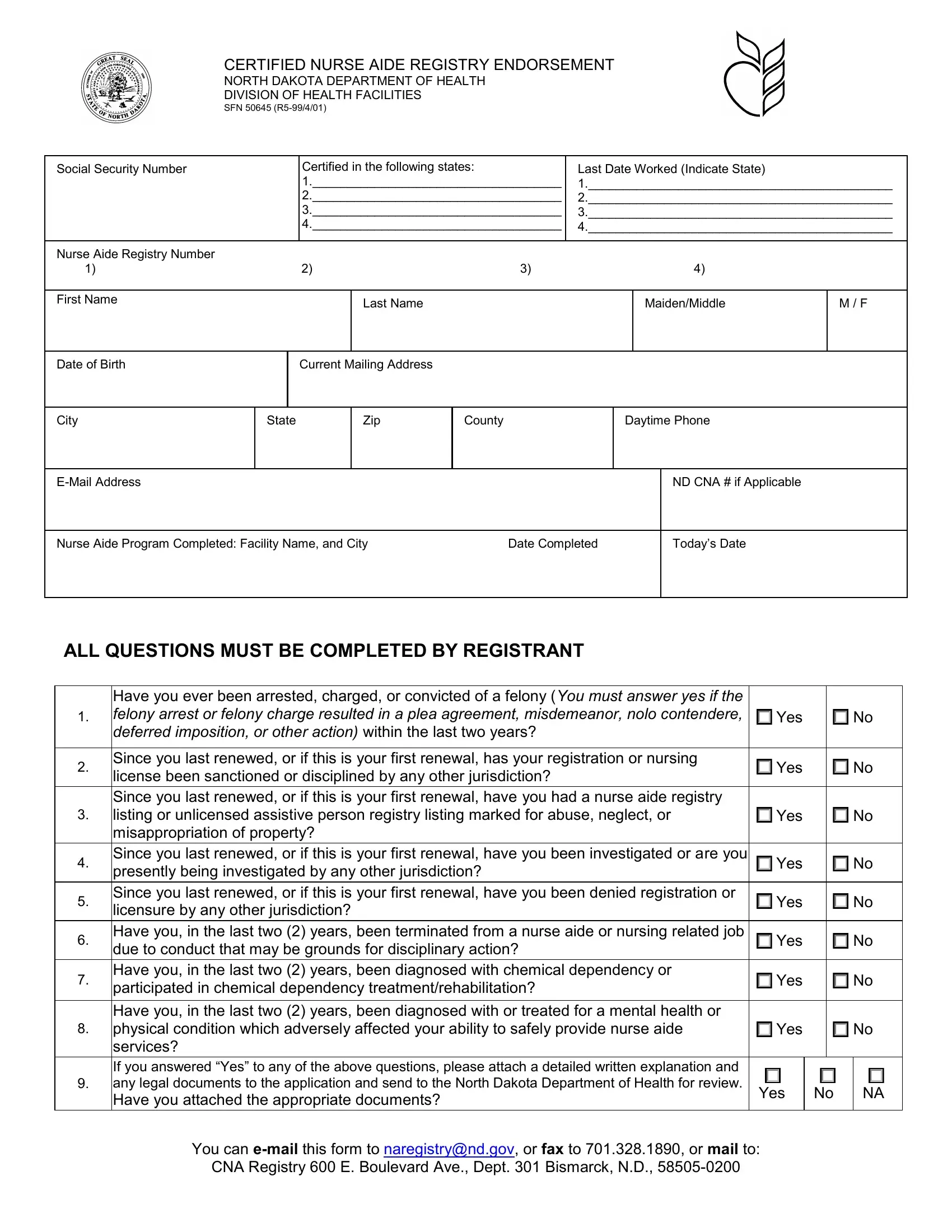
The SFN 50645 form serves as a vital document for Certified Nurse Aides (CNA) seeking endorsement in North Dakota, governed by the Department of Health's Division of Health Facilities. This comprehensive form requests detailed personal information, including social security number, nurse aide registry numbers from other states, and work history, providing a window into the applicant's professional background. Individuals are required to list states where they are certified, along with the date they last worked in those states, ensuring a thorough understanding of their work history. Additionally, the form asks for basic personal details such as name, birth date, and contact information, ensuring the department can maintain proper communication with the applicant. Key sections probe into the applicant's legal history, specifically asking about any felonies, disciplinary actions, or investigations related to their profession in the last few years. This scrutiny extends to inquiries about chemical dependency, mental health, or physical conditions that could impact their ability to safely perform their duties. The directive that all questions must be answered truthfully reinforces the importance of integrity in the application process. Moreover, the option to submit additional documentation for review underscores the commitment of the North Dakota Department of Health to evaluate each candidate thoroughly, ensuring only qualified individuals are endorsed. The form's design to facilitate email, fax, or mail submission accommodates different preferences for submission, underscoring its user-centric approach. Overall, the SFN 50645 form embodies a critical step for nurse aides aiming to extend their practice to North Dakota, encapsulating a rigorous vetting process to uphold high standards in healthcare professionalism and patient safety.
| Question | Answer |
|---|---|
| Form Name | Form Sfn 50645 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | web_endorsement _form_ _fillable_ _savable north dakota cna registry in the mail form |