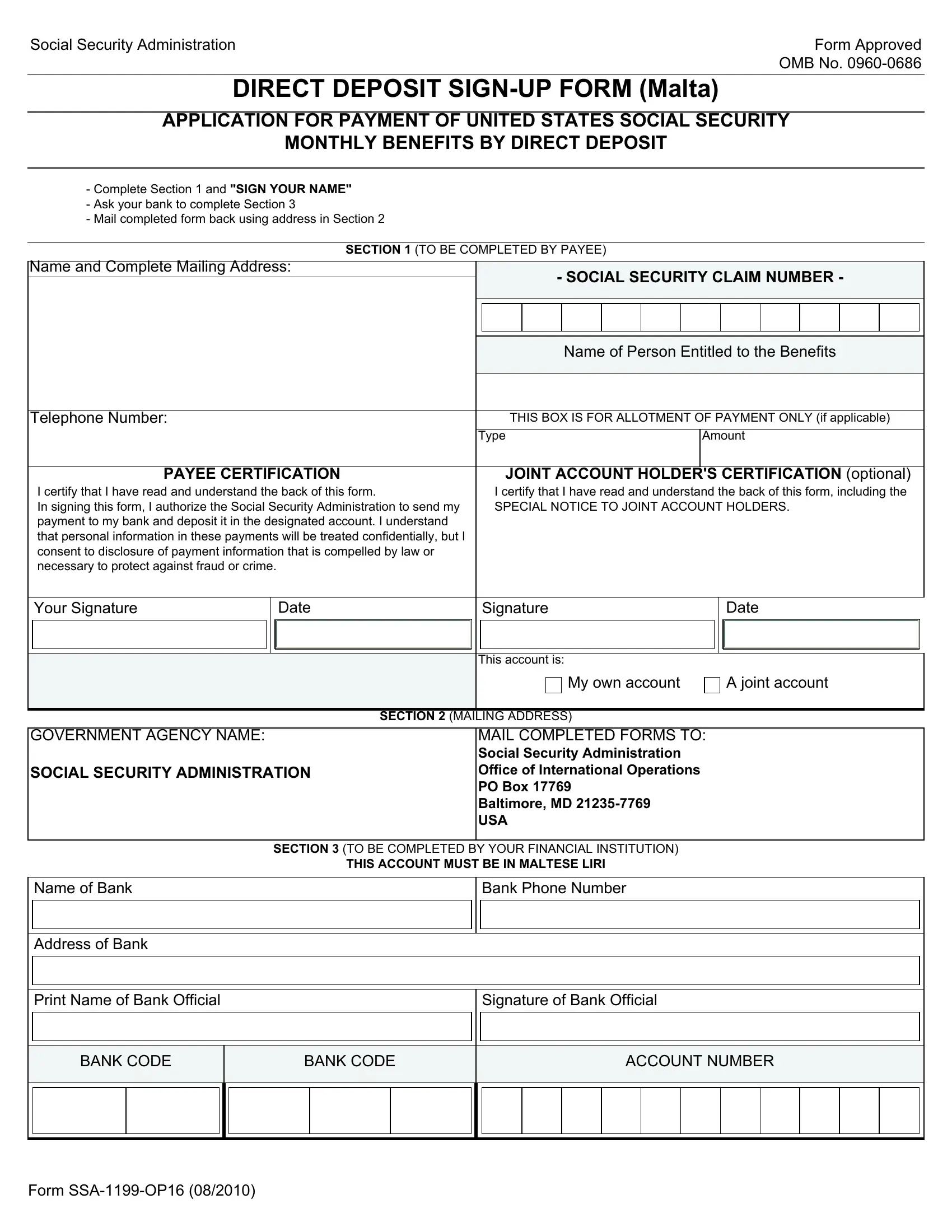
Navigating the complexities of receiving United States Social Security benefits while living abroad can seem daunting, but the SSA-1199-OP16 form, specifically crafted for individuals residing in Malta, simplifies the process by establishing a direct deposit system for monthly benefits. This form requires collaboration between the beneficiary and their bank and involves a straightforward three-section completion process. Initially, beneficiaries are tasked with filling out personal and payment details, followed by a bank section to be filled by the financial institution, ensuring the payments are deposited in Maltese Liri. Moreover, this form comes with provisions for handling joint accounts, emphasizing the importance of promptly reporting any changes, such as address modifications or the death of a joint account holder, to the Social Security Administration or the American Embassy. This procedural safeguard helps prevent the misallocation of funds and ensures compliance with legal and regulatory obligations. The form itself is a testament to the SSA's commitment to providing secure and efficient access to benefits for U.S. citizens living abroad, incorporating precautions against fraud and emphasizing immediate access to funds, thereby offering a dependable financial lifeline for beneficiaries.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 1199 Op16 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Veneto, ssa 1199 form, SSA-1199-OP16, MALTESE |