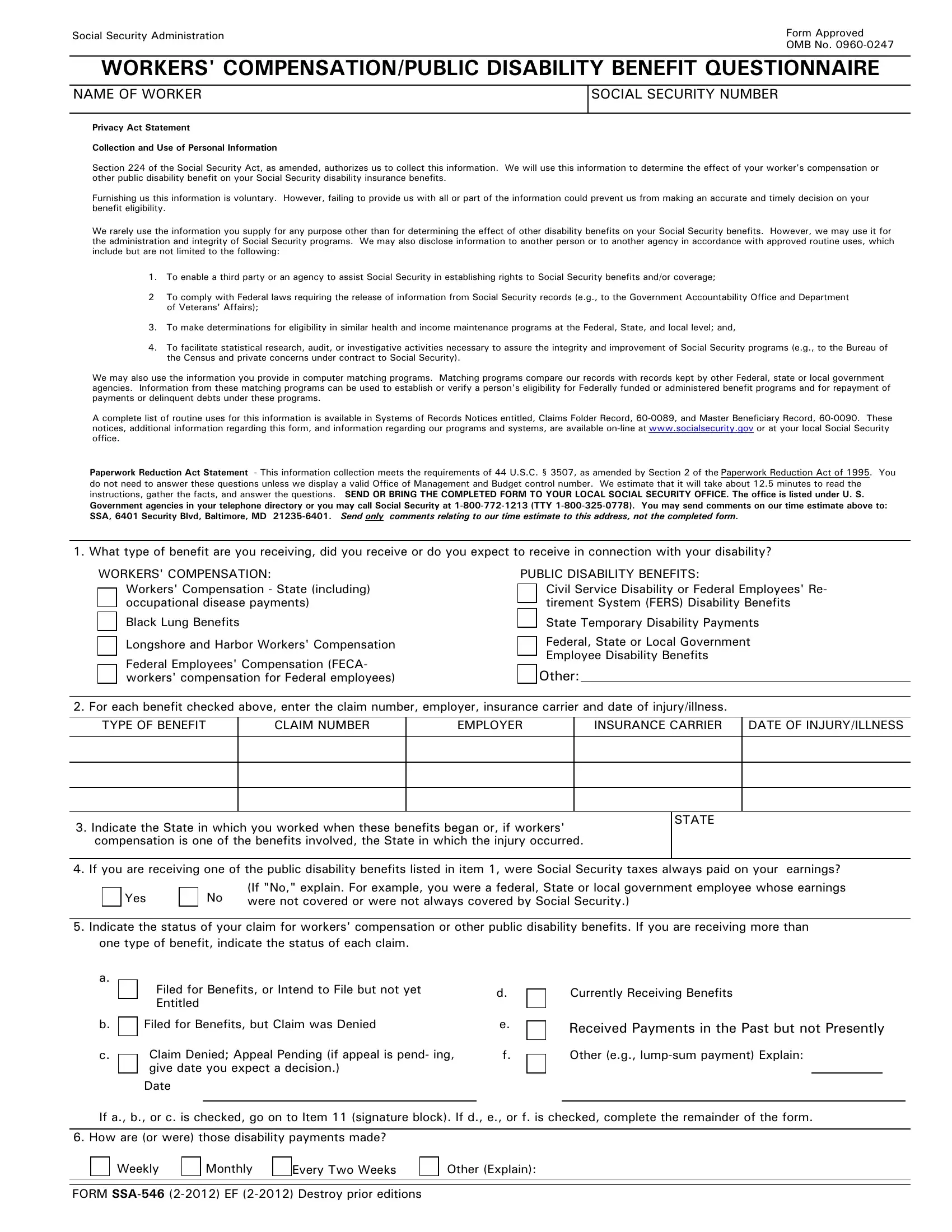
The understanding and management of the SSA-546 form, officially recognized by the Social Security Administration (SSA), play a pivotal role in the lives of individuals seeking to disclose their workers' compensation or public disability benefits within the framework of their Social Security disability insurance benefits. Structured as a questionnaire, this document meticulously gathers pertinent details including the nature of the benefits being received, whether they stem from workers' compensation schemes across various jurisdictions such as state, federal, or specific occupational disease payments, or from a range of public disability benefits encompassing civil service disability or retirement system benefits, to name a few. The comprehensive scope of this form does not merely confine itself to the aggregation of claim-related information; it extends to facilitating a nuanced understanding of how these external disability benefits might influence one's Social Security benefits. Integral to this process is the adherence to the Privacy Act and Paperwork Reduction Act, underscoring the voluntary yet essential nature of providing complete and accurate information to avoid hampering the determination of benefits eligibility. The SSA-546 form further delineates the procedural norms for submitting this information, alongside emphasizing the legal and ethical implications of providing falsified data, thereby ensuring the integrity of the information submitted and safeguarding the rights of the individual within the disability benefits framework.
| Question | Answer |
|---|---|
| Form Name | Form Ssa 546 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form 546 compensation, social security form 546, ssa 546, social security 546 |