
Whenever you would like to fill out BYB, you don't need to download and install any kind of programs - just give a try to our online PDF editor. Our editor is constantly developing to present the very best user experience possible, and that is due to our resolve for continual improvement and listening closely to comments from users. Here is what you would need to do to get going:
Step 1: Press the orange "Get Form" button above. It will open up our tool so you could start filling out your form.
Step 2: With this advanced PDF editing tool, it is possible to do more than simply fill out blank fields. Edit away and make your docs seem high-quality with customized textual content added, or fine-tune the original input to perfection - all that backed up by the capability to incorporate just about any images and sign the document off.
Filling out this form needs care for details. Make sure that all mandatory fields are filled in correctly.
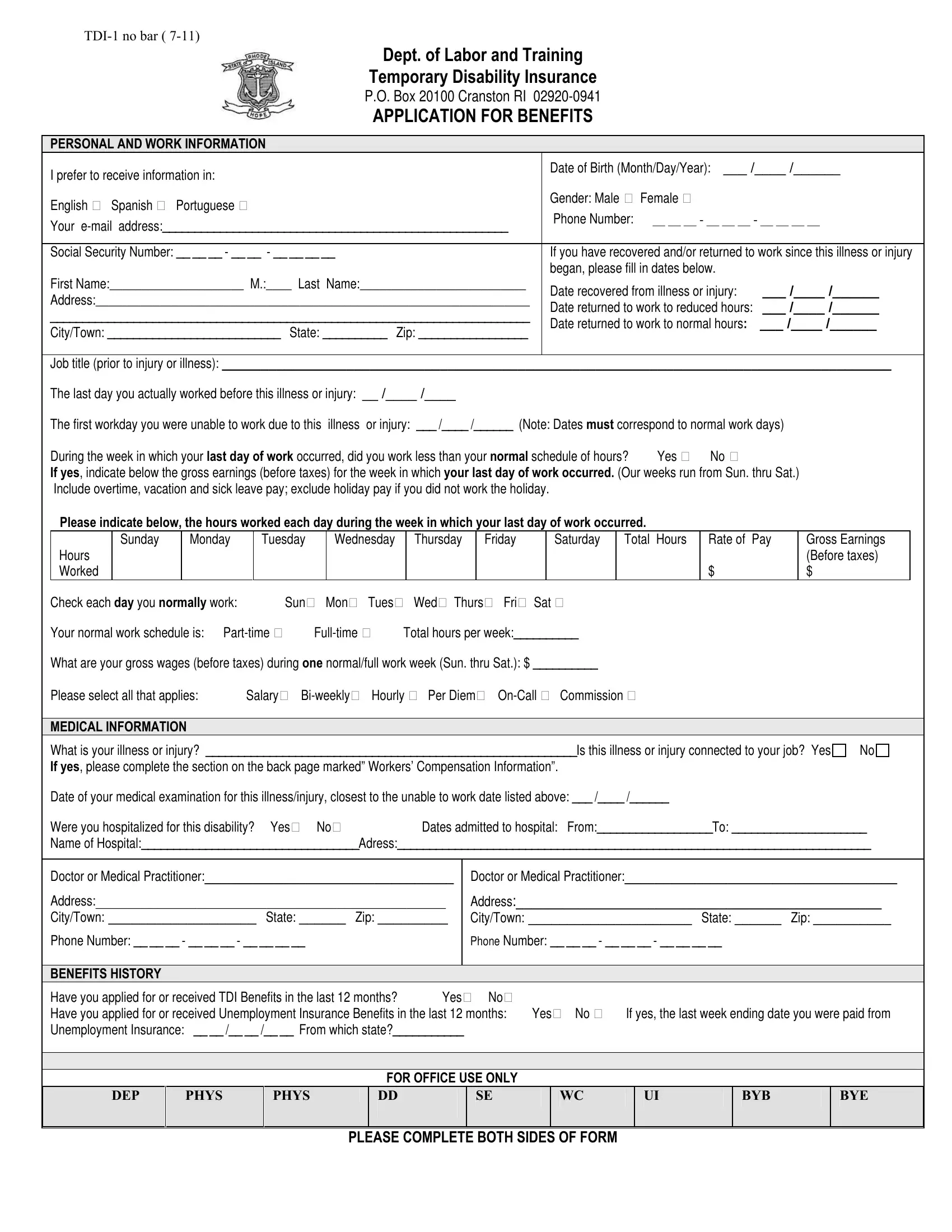
1. It's essential to fill out the BYB correctly, hence be careful while working with the parts containing all these blanks:
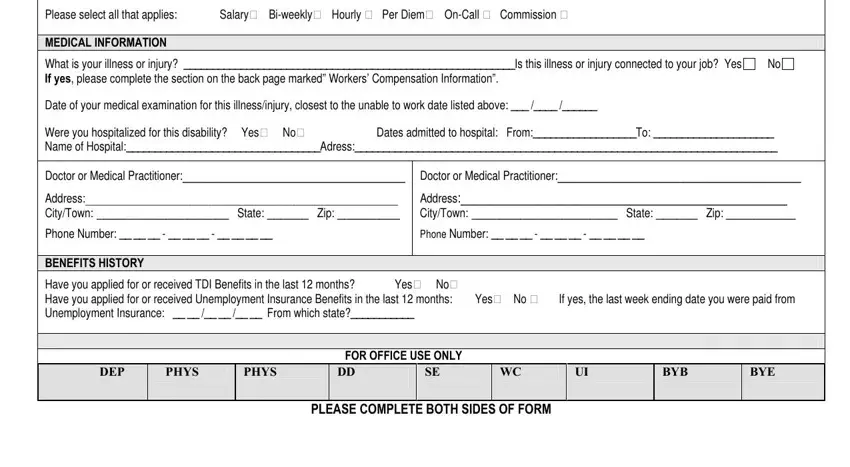
2. Just after the previous selection of fields is done, go to enter the suitable details in these: Check each day you normally work, What is your illness or injury Is, Doctor or Medical Practitioner, Doctor or Medical Practitioner, Address CityTown State Zip, Address CityTown State Zip, Phone Number BENEFITS, Phone Number, Have you applied for or received, DEP, PHYS, PHYS, BYB, BYE, and FOR OFFICE USE ONLY.
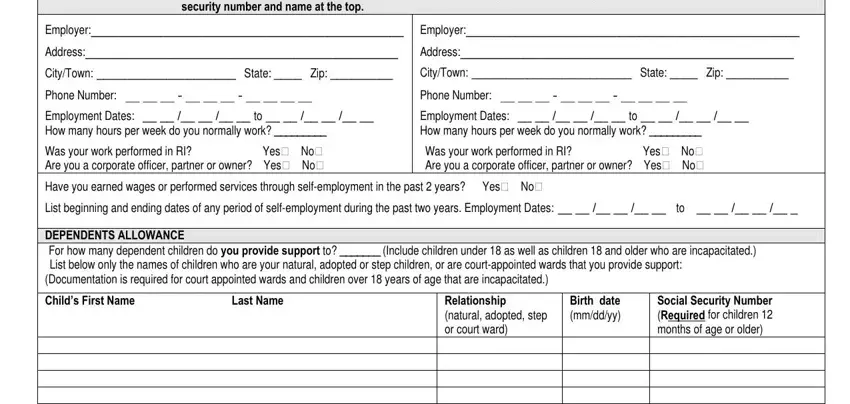
3. Completing EMPLOYER INFORMATION Please, Employer, Employer, Address, Address, CityTown State Zip, CityTown State Zip, Phone Number, Phone Number, Have you earned wages or performed, Childs First Name Last Name, Relationship natural adopted step, Birth date mmddyy, and Social Security Number Required is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. It is time to complete this fourth form section! In this case you will have all of these Relationship natural adopted step, Social Security Number Required, Do you have legal custody of all, Social Security Number, Is any other person claiming your, If yes indicate the name address, Social Security Number, If any legal dependent named above, Name Incapacity Type WORKERS, Have you filed a Workers, If yes please provide the contact, If you have a lawyer representing, Address, and CityTown State Zip blanks to fill out.
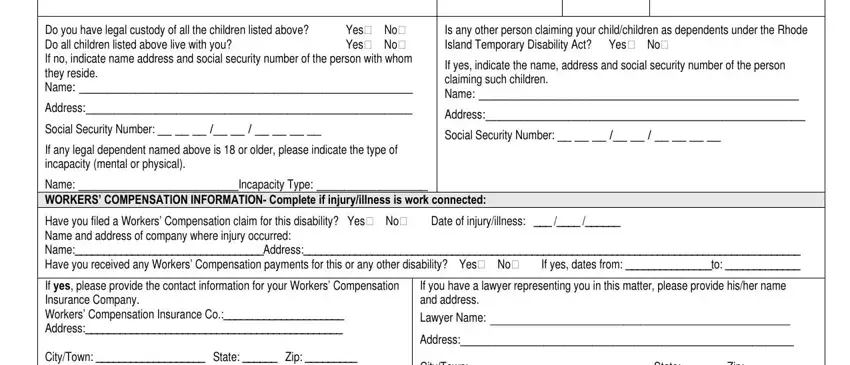
Always be really mindful when completing Social Security Number Required and Address, since this is the part where a lot of people make mistakes.
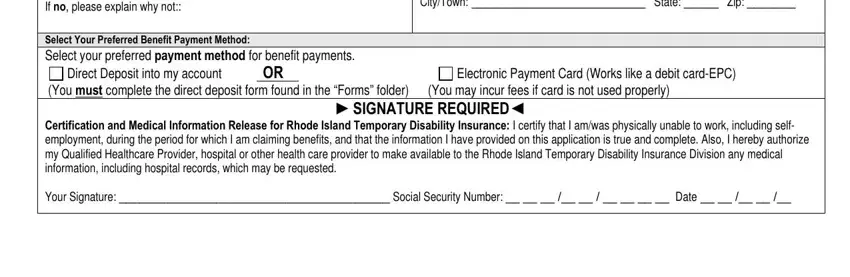
5. The document needs to be finished with this part. Below you will find a comprehensive list of form fields that need appropriate details to allow your document usage to be complete: If yes please provide the contact, Direct Deposit into my account OR, Electronic Payment Card Works like, SIGNATURE REQUIRED, CityTown State Zip, and Certification and Medical.
Step 3: Check the details you've typed into the blank fields and then hit the "Done" button. Join FormsPal today and instantly get access to BYB, set for download. All changes made by you are saved , meaning you can edit the pdf further as required. FormsPal ensures your data confidentiality by using a secure system that in no way saves or shares any kind of private information provided. Be confident knowing your documents are kept safe any time you use our editor!