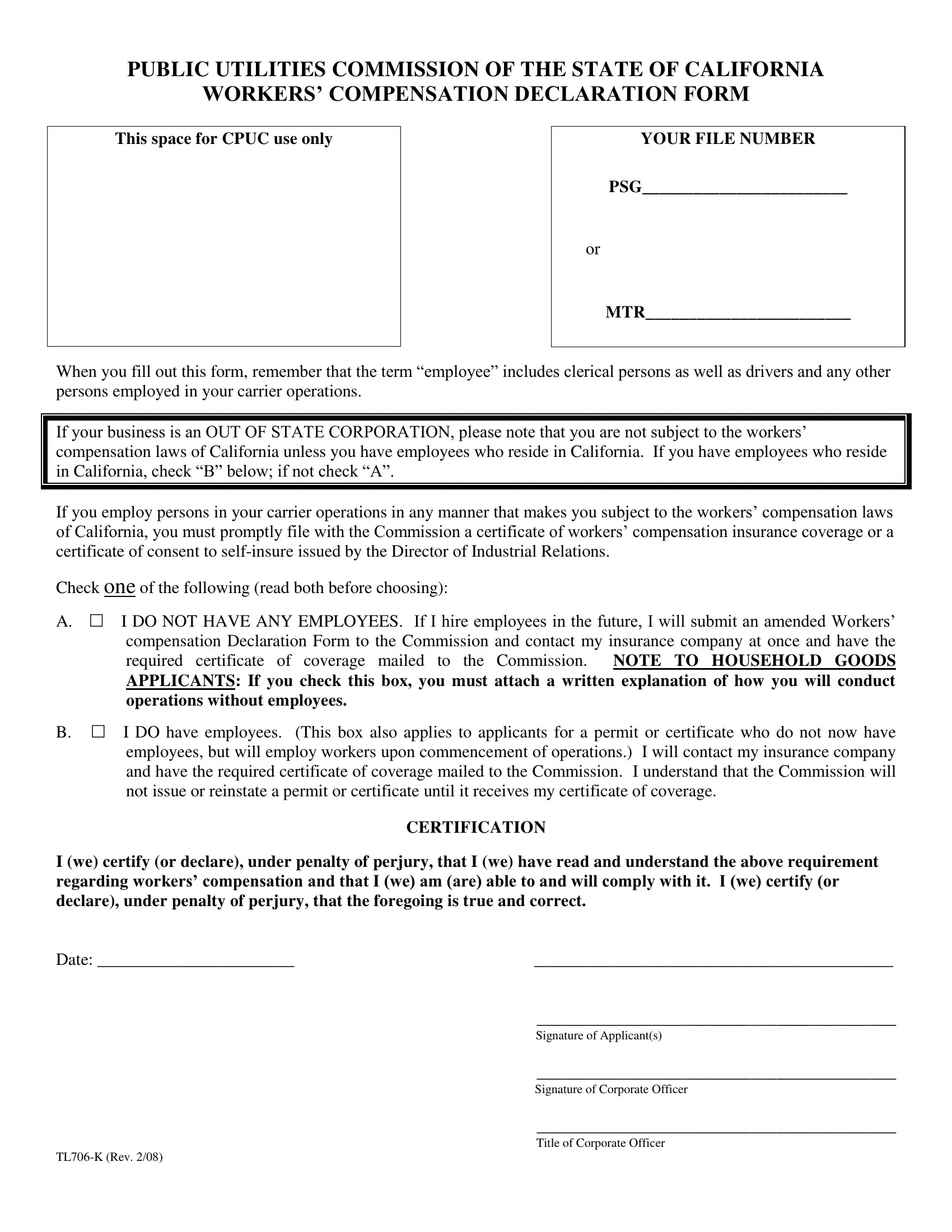
Navigating the complexities of regulatory compliance is essential for businesses in the transportation sector, particularly those regulated by the Public Utilities Commission of the State of California. A crucial component of this compliance is the Workers’ Compensation Declaration Form, known as the TL706 K form. This document serves a dual purpose: it is an affirmation of a business’s adherence to California's workers' compensation laws and a prerequisite for the commission to issue or reinstate permits or certificates for operation. Organizations must disclose whether they have employees and, if so, confirm that they have secured the requisite workers' compensation insurance coverage or an equivalent self-insurance authorization. This form is especially critical for out-of-state corporations operating in California, as their obligation to adhere to the state’s workers’ compensation laws is contingent upon employing residents of California. Essentially, the TL706 K form is a bridge between regulatory compliance and operational authorization, reminding businesses of their responsibility to protect their employees and ensuring that all parties understand the terms of engagement under California law.
| Question | Answer |
|---|---|
| Form Name | Form Tl706 K |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form tl 706k llc, tl 706k form, public utilities commission, fill out tl form |
PUBLIC UTILITIES COMMISSION OF THE STATE OF CALIFORNIA
WORKERS’ COMPENSATION DECLARATION FORM
This space for CPUC use only |
YOUR FILE NUMBER |
PSG________________________
or
MTR________________________
When you fill out this form, remember that the term “employee” includes clerical persons as well as drivers and any other persons employed in your carrier operations.
If your business is an OUT OF STATE CORPORATION, please note that you are not subject to the workers’
compensation laws of California unless you have employees who reside in California. If you have employees who reside in California, check “B” below; if not check “A”.
If you employ persons in your carrier operations in any manner that makes you subject to the workers’ compensation laws of California, you must promptly file with the Commission a certificate of workers’ compensation insurance coverage or a
certificate of consent to
Check one of the following (read both before choosing):
A.I DO NOT HAVE ANY EMPLOYEES. If I hire employees in the future, I will submit an amended Workers’ compensation Declaration Form to the Commission and contact my insurance company at once and have the
required certificate of coverage mailed to the Commission. NOTE TO HOUSEHOLD GOODS
APPLICANTS: If you check this box, you must attach a written explanation of how you will conduct operations without employees.
B.I DO have employees. (This box also applies to applicants for a permit or certificate who do not now have
employees, but will employ workers upon commencement of operations.) I will contact my insurance company and have the required certificate of coverage mailed to the Commission. I understand that the Commission will not issue or reinstate a permit or certificate until it receives my certificate of coverage.
CERTIFICATION
I (we) certify (or declare), under penalty of perjury, that I (we) have read and understand the above requirement regarding workers’ compensation and that I (we) am (are) able to and will comply with it. I (we) certify (or
declare), under penalty of perjury, that the foregoing is true and correct.
Date: _______________________ |
__________________________________________ |
|
__________________________________________ |
|
Signature of Applicant(s) |
|
__________________________________________ |
|
Signature of Corporate Officer |
|
__________________________________________ |
|
Title of Corporate Officer |
|