The administrative landscape of professional credentialing within New York State's health and substance abuse sector is meticulously mapped out through a document known as the TRS 53 form. At the very core, this form represents a critical process for individuals seeking credentials to work in fields related to alcoholism and substance abuse services overseen by the New York State Office of Alcoholism and Substance Abuse Services (OASAS). It initiates with providing essential personal information, pivoting towards a vital consent for a criminal background check—a checkpoint not just a formality but a comprehensive vetting leveraging criminal history information from both the New York State Division of Criminal Justice Services (DCJS) and the Federal Bureau of Investigation (FBI). The provisions laid out articulate a dual purpose: safeguarding the integrity of the credentialing process while ensuring the individual's rights through a protocol for information review and correction. The form also underscores the confidential nature of the acquired information, aligning with federal and state laws. Moreover, it insists on the veracity of the information provided by the applicant, hence embedding accountability within the submission process. Ultimately, the TRS 53 form encapsulates a rigorous screening mechanism, engaging multiple layers of legal, ethical, and procedural considerations, all aimed at bolstering the quality and safety of alcoholism and substance abuse services in New York State.
| Question | Answer |
|---|---|
| Form Name | Form Trs 53 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CASAC, 23-A, DCJS, cbcoasas |
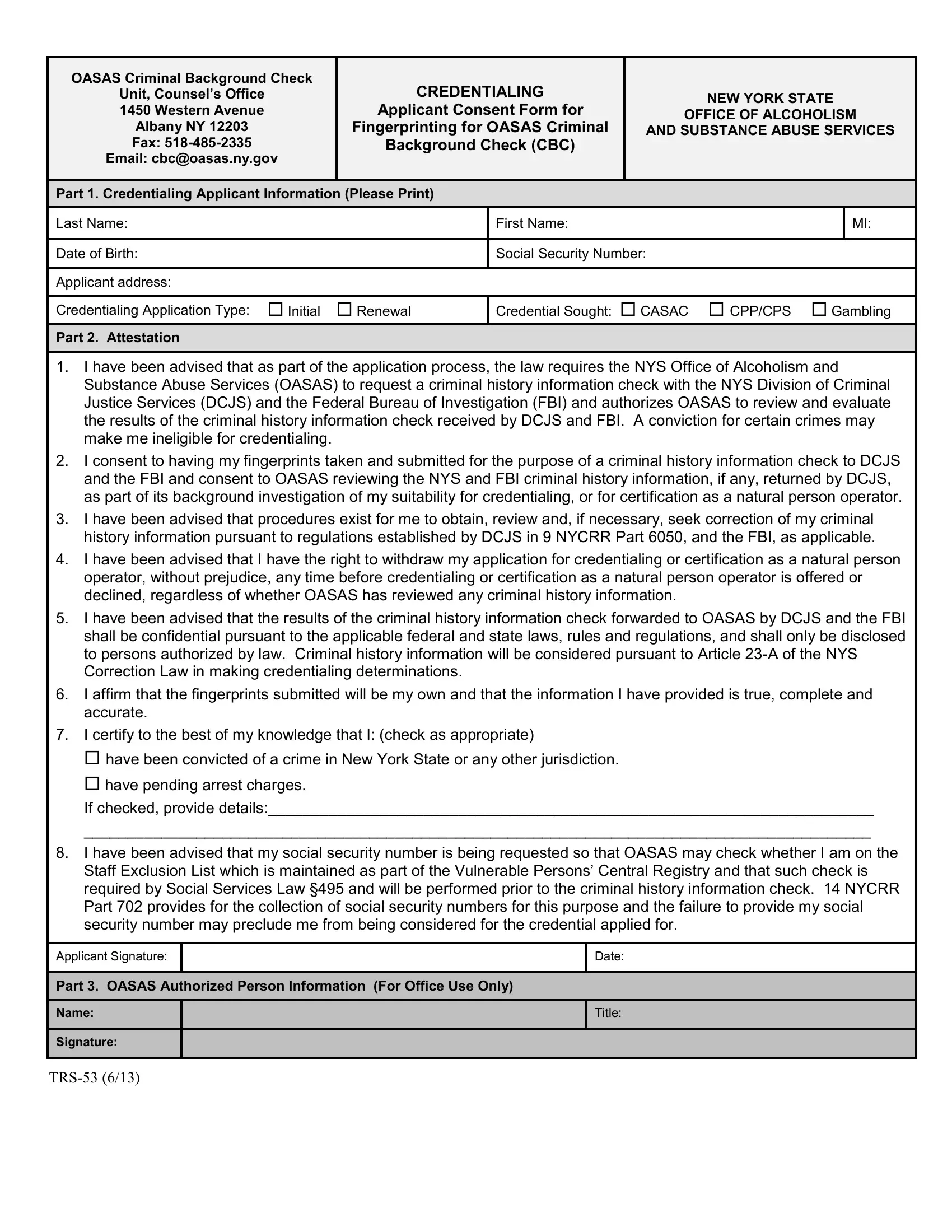
OASAS Criminal Background Check
Unit, Counsel’s Office
1450 Western Avenue
Albany NY 12203
Fax:
Email: cbc@oasas.ny.gov
CREDENTIALING
Applicant Consent Form for
Fingerprinting for OASAS Criminal
Background Check (CBC)
NEW YORK STATE
OFFICE OF ALCOHOLISM
AND SUBSTANCE ABUSE SERVICES
Part 1. Credentialing Applicant Information (Please Print)
Last Name: |
First Name: |
|
MI: |
|
|
|
|
Date of Birth: |
Social Security Number: |
|
|
|
|
|
|
Applicant address: |
|
|
|
|
|
|
|
Credentialing Application Type: Initial Renewal |
Credential Sought: CASAC CPP/CPS |
Gambling |
|
Part 2. Attestation
1.I have been advised that as part of the application process, the law requires the NYS Office of Alcoholism and Substance Abuse Services (OASAS) to request a criminal history information check with the NYS Division of Criminal Justice Services (DCJS) and the Federal Bureau of Investigation (FBI) and authorizes OASAS to review and evaluate the results of the criminal history information check received by DCJS and FBI. A conviction for certain crimes may make me ineligible for credentialing.
2.I consent to having my fingerprints taken and submitted for the purpose of a criminal history information check to DCJS and the FBI and consent to OASAS reviewing the NYS and FBI criminal history information, if any, returned by DCJS, as part of its background investigation of my suitability for credentialing, or for certification as a natural person operator.
3.I have been advised that procedures exist for me to obtain, review and, if necessary, seek correction of my criminal history information pursuant to regulations established by DCJS in 9 NYCRR Part 6050, and the FBI, as applicable.
4.I have been advised that I have the right to withdraw my application for credentialing or certification as a natural person operator, without prejudice, any time before credentialing or certification as a natural person operator is offered or declined, regardless of whether OASAS has reviewed any criminal history information.
5.I have been advised that the results of the criminal history information check forwarded to OASAS by DCJS and the FBI shall be confidential pursuant to the applicable federal and state laws, rules and regulations, and shall only be disclosed to persons authorized by law. Criminal history information will be considered pursuant to Article
6.I affirm that the fingerprints submitted will be my own and that the information I have provided is true, complete and accurate.
7.I certify to the best of my knowledge that I: (check as appropriate)
have been convicted of a crime in New York State or any other jurisdiction.
have pending arrest charges.
If checked, provide details:______________________________________________________________________
___________________________________________________________________________________________
8.I have been advised that my social security number is being requested so that OASAS may check whether I am on the Staff Exclusion List which is maintained as part of the Vulnerable Persons’ Central Registry and that such check is required by Social Services Law §495 and will be performed prior to the criminal history information check. 14 NYCRR Part 702 provides for the collection of social security numbers for this purpose and the failure to provide my social security number may preclude me from being considered for the credential applied for.
Applicant Signature:
Date:
Part 3. OASAS Authorized Person Information (For Office Use Only)
|
Name: |
|
|
|
Title: |
|
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature: