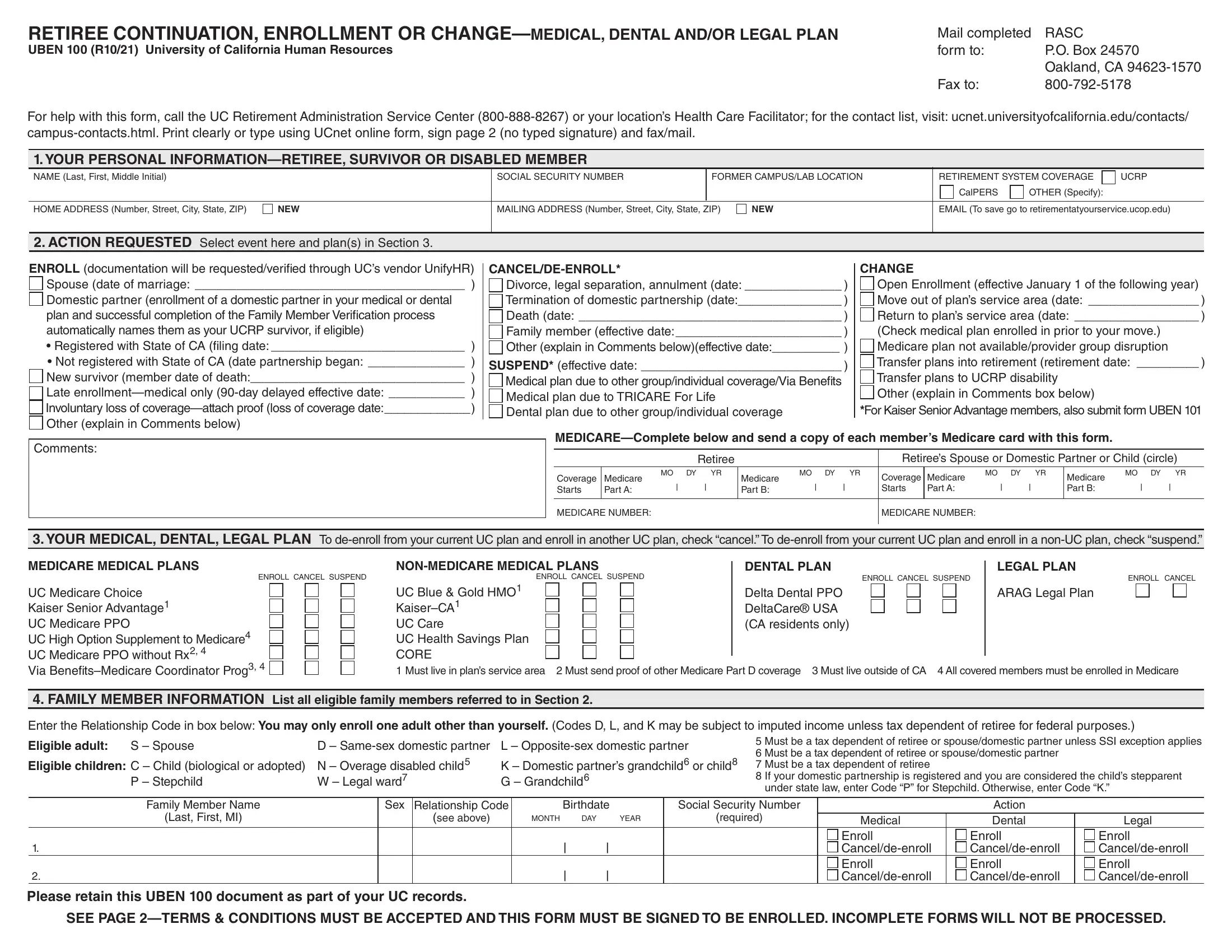
Navigating the dynamics of retirement, particularly in the context of health, dental, and legal plan enrollments or changes, demands a keen awareness of the processes and forms involved. Within the framework of the University of California Human Resources, the RASC UBEN 100 form plays a crucial role. This document, designated for retiree continuation, enrollment, or adjustments to medical, dental, and/or legal plans, serves as a vital tool for those stepping into or navigating their retirement phase. The form's purpose extends to facilitating a transition or alteration in the coverage landscape for retirees, their spouses, or dependents, accommodating a variety of circumstances from new enrollments to changes in personal information or plan adjustments predicated on significant life events. It underscores the procedural steps needed to address coverage under Medicare, detailing a process that encompasses submitting personal details, specifying the type of action requested—be it enrollment, cancellation, or a plan switch—and meticulously outlining the terms for medical, dental, and legal plans. Moreover, it encapsulates the eligibility specifics for family members, underpinning the University of California’s commitment to providing a comprehensive guide for its retirees through the intricacies of plan management and adjustments, thereby ensuring a semblance of security and continuity in their post-career life.
| Question | Answer |
|---|---|
| Form Name | Form Uben 100 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | udemy, how to make ube halaya, ubuntu, uben 100 |