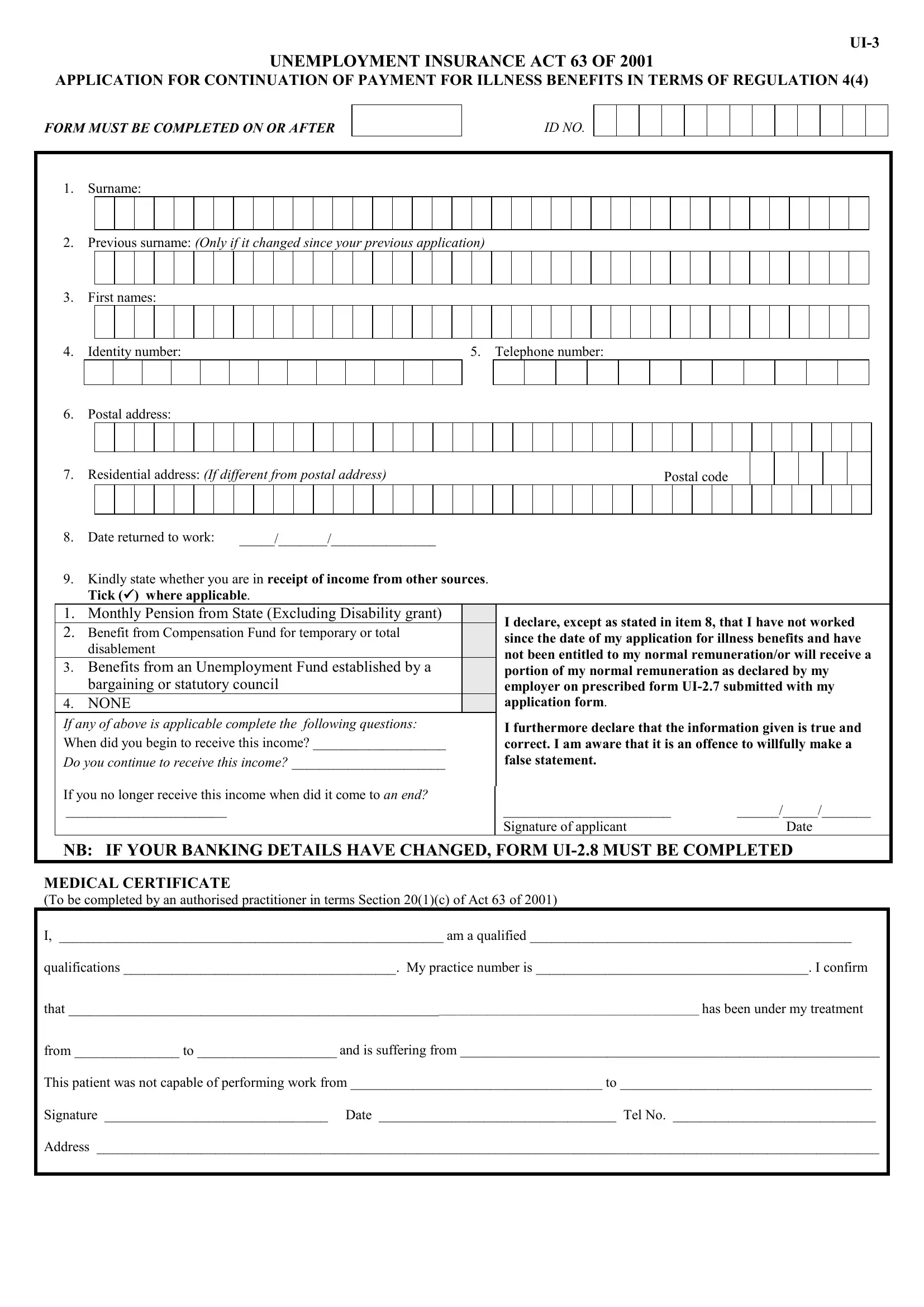
Understanding the intricacies of the UI-3 form can be a crucial step for individuals navigating the complexities of unemployment benefits due to illness. This form, anchored within the Unemployment Insurance Act 63 of 2001, serves as an application for the continuation of payment for illness benefits, following specific regulations. Applicants are required to fill out detailed personal information, including surname changes, identity number, contact details, and residential information. A critical section of the form includes a declaration regarding the receipt of any additional income during the illness period, which encompasses state pensions, benefits from the Compensation Fund, or any unemployment fund contributions. This aspect ensures that payments are accurately determined based on the individual's financial status during their illness. Additionally, the necessity for a medical certificate, completed by an authorized practitioner, underlines the importance of verified medical conditions on the decision process for the continuation of benefits. The form also includes provisions for individuals to update their banking details, ensuring that any payments made are directed to the correct account. Completing the UI-3 form accurately and truthfully is not only a requirement but a legal responsibility, as it includes a declaration of the veracity of the information provided, emphasizing the seriousness of the application process.
| Question | Answer |
|---|---|
| Form Name | Form Ui 3 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | UI-3, ky ui 3 form pdf, disablement, ky ui 3 form |
UNEMPLOYMENT INSURANCE ACT 63 OF 2001
APPLICATION FOR CONTINUATION OF PAYMENT FOR ILLNESS BENEFITS IN TERMS OF REGULATION 4(4)
FORM MUST BE COMPLETED ON OR AFTER
ID NO.
1.Surname:
2.Previous surname: (Only if it changed since your previous application)
3.First names:
4. Identity number: |
5. Telephone number: |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6.Postal address:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Residential address: (If different from postal address) |
|
|
|
|
|
|
|
|
|
Postal code |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
Date returned to work: |
_____/_______/_______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
9. |
Kindly state whether you are in receipt of income from other sources. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
Tick () where applicable. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
1. |
Monthly Pension from State (Excluding Disability grant) |
|
|
I declare, except as stated in item 8, that I have not worked |
|
|||||||||||||||||||||||||||||||||||||||||
2. |
Benefit from Compensation Fund for temporary or total |
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
since the date of my application for illness benefits and have |
|
|||||||||||||||||||||||||||||||||||||||||||
|
disablement |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
not been entitled to my normal remuneration/or will receive a |
|
|||||||||||||||||||||||||||||
3. |
Benefits from an Unemployment Fund established by a |
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
portion of my normal remuneration as declared by my |
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
|
||||||||||||||||||||||||||||||||||||||||||||
|
bargaining or statutory council |
|
|
employer on prescribed form |
|
|||||||||||||||||||||||||||||||||||||||||
4. |
NONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
application form. |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
If any of above is applicable complete the following questions: |
|
I furthermore declare that the information given is true and |
|
|||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
When did you begin to receive this income? ___________________ |
|
correct. I am aware that it is an offence to willfully make a |
|
|||||||||||||||||||||||||||||||||||||||||||
Do you continue to receive this income? ______________________ |
|
false statement. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
If you no longer receive this income when did it come to an end? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
_______________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
________________________ |
|
|
|
______/_____/_______ |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of applicant |
|
|
Date |
|
||||||||||||||||||
NB: IF YOUR BANKING DETAILS HAVE CHANGED, FORM
MEDICAL CERTIFICATE
(To be completed by an authorised practitioner in terms Section 20(1)(c) of Act 63 of 2001)
I, _______________________________________________________ am a qualified ______________________________________________
qualifications _______________________________________. My practice number is _______________________________________. I confirm
that _____________________________________________________________________________________________________ has been under my treatment
from _______________ to ____________________ and is suffering from ____________________________________________________________
This patient was not capable of performing work from ____________________________________ to ____________________________________
Signature ________________________________ Date __________________________________ Tel No. _____________________________
Address ________________________________________________________________________________________________________________