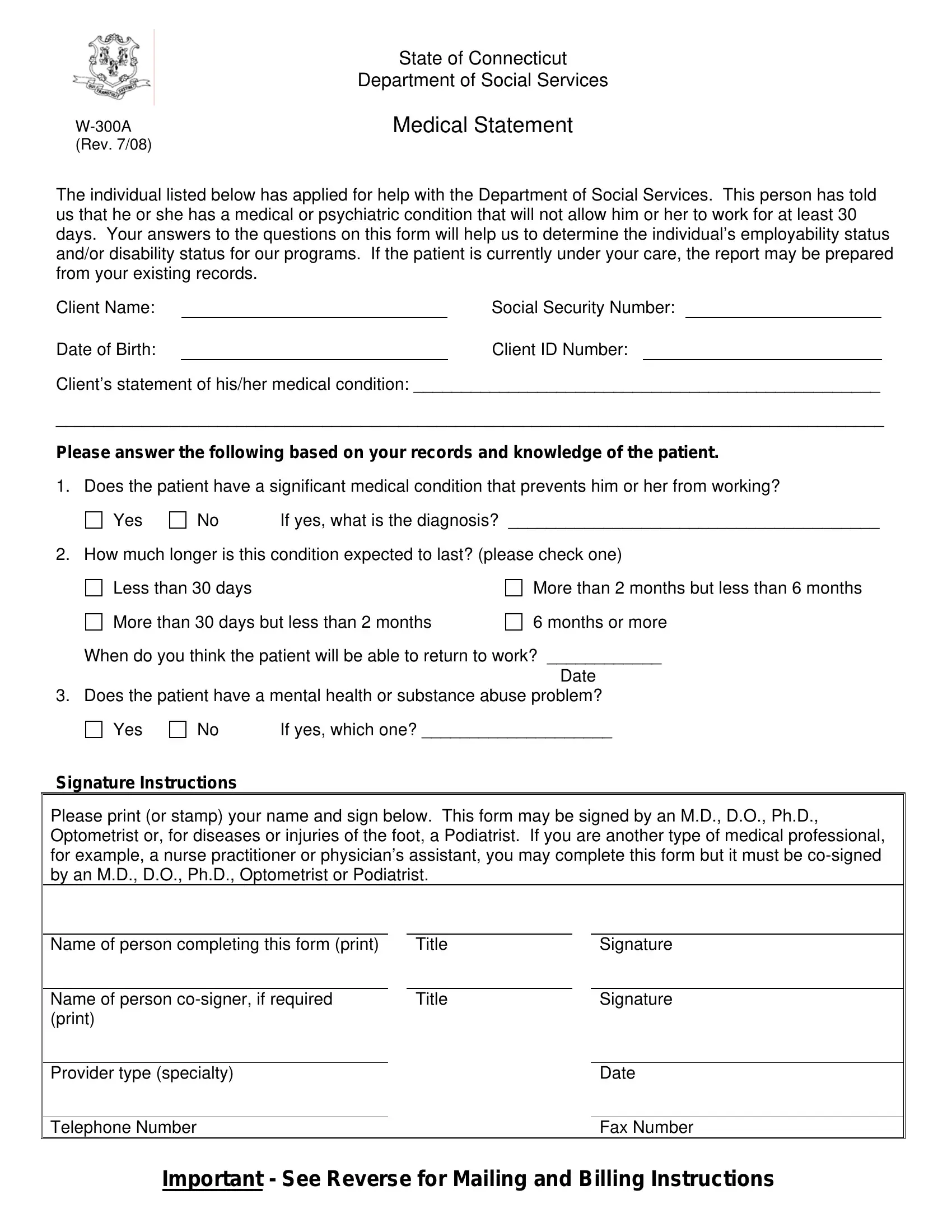
Assistance from the Department of Social Services (DSS) can be a crucial lifeline for individuals facing medical or psychiatric conditions that impede their ability to work. The primary tool for evaluating the need for such assistance is the W-300A Medical Statement, a documentation process set forth by the State of Connecticut's Department of Social Services. Designed to meticulously assess an individual's medical condition and its impact on their employability or disability status, this form requires detailed input from healthcare providers. It delves into specifics: whether the patient is unable to work due to a significant medical or psychiatric condition, the nature of the diagnosis, the expected duration of the impediment, and an estimation of when the individual might return to work. Additionally, the form queries the presence of mental health or substance abuse problems, further tailoring the department's response to the individual's needs. Critical in this process is the accurate and thorough completion of the form by qualified medical professionals—M.D.s, D.O.s, Ph.D.s, optometrists, or podiatrists, with provisions for other medical personnel to contribute under specific conditions. This procedure not only facilitates the appropriate delivery of services but also underscores the collaborative effort between healthcare providers and social services to support individuals facing work-limiting health challenges.
| Question | Answer |
|---|---|
| Form Name | Form W 300A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | dss form w 300a, medical forms for saga cash, saga cash form ct, saga application form |
|
State of Connecticut |
|
Department of Social Services |
Medical Statement |
|
(Rev. 7/08) |
|
The individual listed below has applied for help with the Department of Social Services. This person has told us that he or she has a medical or psychiatric condition that will not allow him or her to work for at least 30 days. Your answers to the questions on this form will help us to determine the individual’s employability status and/or disability status for our programs. If the patient is currently under your care, the report may be prepared from your existing records.
Client Name: |
|
Social Security Number: |
|
|
Date of Birth: |
|
Client ID Number: |
|
|
Client’s statement of his/her medical condition: _________________________________________________
_______________________________________________________________________________________
Please answer the following based on your records and knowledge of the patient.
1. Does the patient have a significant medical condition that prevents him or her from working?
Yes
No |
If yes, what is the diagnosis? _______________________________________ |
2. How much longer is this condition expected to last? (please check one)
Less than 30 days
More than 30 days but less than 2 months
More than 2 months but less than 6 months
6 months or more
When do you think the patient will be able to return to work? ____________
Date
3. Does the patient have a mental health or substance abuse problem?
Yes
No |
If yes, which one? ____________________ |
Signature Instructions
Please print (or stamp) your name and sign below. This form may be signed by an M.D., D.O., Ph.D., Optometrist or, for diseases or injuries of the foot, a Podiatrist. If you are another type of medical professional, for example, a nurse practitioner or physician’s assistant, you may complete this form but it must be
Name of person completing this form (print) |
|
Title |
|
Signature |
|
|
|
|
|
Name of person |
|
Title |
|
Signature |
(print) |
|
|
|
|
|
|
|
|
|
Provider type (specialty) |
|
|
|
Date |
|
|
|
|
|
Telephone Number |
|
|
|
Fax Number |
Important - See Reverse for Mailing and Billing Instructions
Please return this form to:
DSS Worker:
Address:
Telephone: |
|
Fax No. |
Release of Information
Name of Doctor, Clinic or Hospital __________________________________________________
I hereby authorize the medical professional named above to release or disclose to the state of Connecticut, Department of Social Services, the following information:
All medical records or other information regarding my treatment, hospitalization and/or outpatient care for my condition including: psychological and psychiatric impairments, drug and alcohol abuse, sickle cell anemia, AIDS, sexually transmitted diseases, tests for HIV, and how my health problems affect my activities of daily living and my ability to work.
I authorize a photocopy or fax of this release to be accepted with the same authenticity as the original. I understand that I may withdraw this authorization in writing at any time, except for action already taken. Unless I have cancelled it, this authorization will expire when a determination is made with regard to my eligibility for Medicaid disability and/or SAGA unemployability benefits.
__________________________________________ |
_________________________ |
Signature |
Date |
Billing and Payment Instructions
Please access the Automated Eligibility Verification System (AEVS) for confirmation of eligibility.
If SAGA eligibility is confirmed, you will need to be enrolled as a CHNCT provider in order to be paid. Please call CHNCT Provider Relations at (800)
Submit claims for all other eligibility categories to EDS, P.O. Box 2941, Hartford, Ct. 06104. Submit your claim on a CMS 1500 form.
Important: If client is not currently active with DSS, you must attach form