Applying for assistance from the Department of Social Services in Connecticut requires careful completion of the right forms, among which the W-1F form is crucial for particular demographics. Designed to collect necessary information to assess eligibility for a variety of programs, this form caters specifically to single individual households or married couples without dependent children, seeking aid through State Supplement, Medicaid, Food Stamp, State-Administered General Assistance (SAGA), or Home Care for Elders. For households that exceed two persons or those with dependent children, the W-1E form is the appropriate document. The W-1F form simplifies the application process for Food Stamps through the W-IFOOD form and accommodates non-citizens applying solely for Emergency Medicaid without requiring Social Security numbers or citizenship status. Accurate and complete answers are paramount for processing the Special Eligibility Determination Document. Furthermore, this form outlines the necessity of a face-to-face interview, deadlines for submission, and the provision of proofs to substantiate claims made within the application. Importantly, it addresses accommodations for applicants with disabilities, ensuring that all individuals have equitable access to apply for the assistance they need. The W-1F form also serves as a gateway for voter registration, emphasizing the Department of Social Services' commitment to facilitating civic participation among its applicants.
| Question | Answer |
|---|---|
| Form Name | Form W1 F |
| Form Length | 18 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 4 min 30 sec |
| Other names | ct, lnformation, of, cna application form ct |
STATE OF CONNECTICUT - DEPARTMENT OF SOCIAL SERVICES |
|
(Rev. 4/07) |
Instructions for Special Eligibility Determination Document |
|
The purpose of this form is to collect information we need to determine if you are eligible to receive help from the Department of Social Services.
This form may be used only by single individual households or married couples applying for the State Supplement, Medicaid, Food Stamp,
If you are not a citizen and are applying only for Emergency Medicaid, you do not have to provide your Social Security number or citizenship status.
Unless otherwise instructed, be sure to answer all the questions on the form. Answer each question to the best of your ability. If the answer to a question is no, write or check "NO" on the form. If the answer to a question is yes, write or check "YES" and give the details in the space provided. Your answers must be complete and correct so that we may process your Special Eligibility Determination Document properly.
If you cannot do something we ask you to do because you have a disability, you may request an accommodation or special help. We can use different methods to complete your application. For example, we may be able to complete your application over the telephone if you cannot come into the office, we may be able to help you get certain proofs, or give you extra time to provide information. If we do not agree to provide an accommodation or special help, you can complain to the department's Americans with Disabilities Act (ADA) coordinator. See the bottom of page 14 for how to make a complaint.
You can also have another person apply for Food Stamps for you or get an EBT card to buy your food. You may have someone else help you complete the form. If someone else does help you, be sure that the helper signs and dates the last page of the form. Be sure that you sign and date the form as well.
/I |
The program(s) for which you are applying require that you have a |
||||
for |
at |
. Complete this form and bring it with you to the interview. |
|||
|
|||||
/ |
Mail or bring in your completed application form to this office no later than |
. If you bring this form in, be |
|||
sure to call your worker for an appointment first. |
|
|
|||
|
|
|
|||
Please try to bring in or mail the required proofs with the application form. However, if you do not have all the proofs, please keep your appointment or mail the form in before the deadline with whatever information you do have. If you do not appear for your interview the department will not automatically schedule a second appointment. You will have to contact the department to reschedule an appointment.
IF YOU HAVE ANY QUESTIONS, PLEASE CALL YOUR ELIGIBILITYWORKER, |
9 |
AT |
|
To Home Care applicants: You must call our Alternate Care Unit at
THIS INFORMATION IS AVAILABLE IN ALTERNATE FORMATS. PHONE (800) |
I OFFICE ADDRESS |
(800) |
|
(See Reverse Side for Information about Required Proofs and Processing Time Limits) |
I |
|

Certain information that you have given in your Special Eligibility 'Determination Document must be verified before the department can grant assistance. The following list will give you an idea of the documents that may be used to prove your statements.
Household Members - You may use copies of birth certificates, baptismal records or other records documenting birthdates and relationships, marriage and divorce papers, or school attendance verification for children over age 18.
Income - You may provide copies of pay stubs, tax returns or bookkeeping records for
Assets - You may use bankbooks, bank statements, trust fund agreements, copies of stockslbondslU.S. Savings bonds, life insurance policies, a letter from a financial institution, a copy of a car registration, deeds or legal agreements as proof.
Shelter and Utilitv Costs - These may be proved by giving your worker your latest rent receipt, a copy of your lease, a copy of your utility bill, a letter from your landlord, a copy of your mortgage bill, a copy of your property tax bill or a copy of your homeowner's insurance.
Medical Insurance and Expenses - Medical insurance policies, medical cards and copies of medical bills may be used to prove these expenses.
Child Support Costs - You may provide a copy of the court order to prove the legal obligation to pay child support and the obligated amount. Acceptable forms of proof of your actual payments include such documents as cancelled checks, wage withholding statements, or a statement from the custodial parent as to the amount you pay in child support or the child support expected to be paid within the certification period.
Students - Acceptable proofs are items such as a signed School Verification Letter
Other -
EXPEDITED SERVICE, EMERGENCY BENEFITS AND PROCESSING TIME LIMITS
We are required to make a determination of eligibility within certain time limits. If you are applying for a money payment or for medical assistance under a Public Assistance program, we must decide if you qualify and, if you are eligible, issue benefits within 45 days unless you are applying for a disability benefit. In that case we must decide and, if you are eligible, issue benefits within 90 days.
For Food Stamp applications, we must decide if you qualify and, if you are eligible, provide you with benefits within 30 days. If your situation is such that you have no, or almost no, income or assets, we are required to decide if you qualify and provide you with expedited service Food Stamp Benefits within seven days. You may also qualify for EXPEDITED SERVICE Food Stamp benefits if your monthly shelter expenses are more than your gross income and assets, or you are a destitute migrant or seasonal farm worker.
For
4days.
If you need food or medical assistance before we decide if you qualify for benefits, or if your circumstances are such that you are in an EMERGENCY SITUATION and your needs are not being met by another source, contact your eligibility worker. Examples of these emergency situations include those in which there is an immediate need for medical treatment and you don't have a medical card, or you have no money and there is a threat of serious harm as a result.
If we know about your emergency, we can give your application a priority in deciding if you qualify. Each office has a client representative who will work with your eligibility worker in emergency situations to help make sure you get benefits quickly if it is possible. We cannot provide benefits to you, however, until we have all the information we need to make the decision that you do, in fact, qualify.
If you need legal help with your application contact your Statewide Legal Services office at
The Department of Social Services
Offers Voter Registration
The department wants you to have the chance to be active in the political process.
Congress passed the National Voter Registration Act (NVRA) of 1993 in order to make it easier for you to get and file an application to register to vote. The Department of Social Services can help you register to vote. That is why we ask you to answer the questions on the next page. These questions tell us about whether you are registered to vote. Please complete this form and return it to us with your application form.
If you are not registered to vote, you can apply to register with the department. You need to fill out an application to register. We sent an application to register to you with this application form or your worker gave you a form. If you did not receive an application to register to vote, please tell your worker. Your worker will get a form to you.
-
8 2
c
g %
Y
3
I? ~F
2 8. 2
(D ;$.g
ZA 3
2 0 2 g
l u 3 3
0
2 a 3 3 N M 2 E-
3 3
2 $ 0 3
o a g
rSg S q . 3
3 $ 2 -
gcj n e g
v -0 $ 3.
$ 6 8 5 . 5
?'3 - a -
2 3 . (D -
-
i 3 G .A- Z
03 A
$ 0 8
0 0 -
T D 2
h
CX, 2. 2
8
I
I
I
I
I
I
I
I
hI
4 ;
X I
2
9, I
3
a lI
$ I
DECLINING TO REGISTER TO VOTE
Connecticut General Statutes Sec.
If you are not registered to vote where you live now, would you like to apply to register to vote here today?
Yes |
No |
I decline because I am already registered |
IF YOU DO NOT CHECK A BOX, YOU WILL BE CONSIDERED TO HAVE DECIDED NOT TO REGISTER TO VOTE AT THIS TIME.
Applying to register or declining to register will not affect the assistance this agency will provide.
If you would like help filling out the voter registration application form, we will help you. The decision whether to seek or accept help is yours.
If you are applying in person, you may fill out the application form in private.
If you are applying by mail, call your worker. A notice is included that has your worker's name and telephone number.
If you fill out and sign the voter registration application, you can:
leave it with your worker,
mail it to us in the enclosed envelope or
mail it directly to the registrar of voters in your Town Hall.
0 0
A G S
0 <
$ 2
Y
0 Y
5 g
7
2 2.
rc
W - I F |
|
STATE OF CONNECTICUT |
|
|
(Rev. 4/07) |
|
DEPARTMENT OF SOCIAL SERVICES |
|
|
|
|
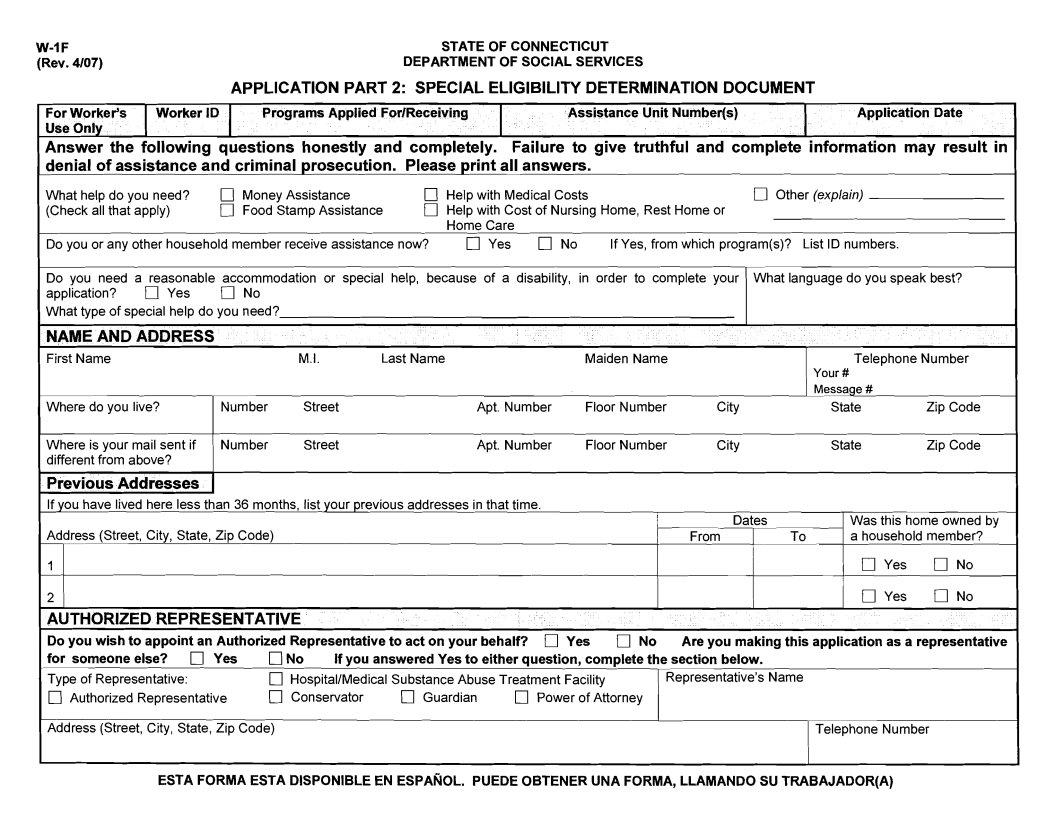
APPLICATION PART 2: SPECIAL ELIGIBILITY DETERMINATION DOCUMENT |
|
|
For Worker's |
Worker ID |
Programs Applied ForlReceiving |
Assistance Unit Number(s) |
Application Date |
Use Only |
|
|
|
|
Answer the following questions honestly and completely. Failure to give truthful and complete information may result in denial of assistance and criminal prosecution. Please print all answers.
What help do you need? |
Money Assistance |
Help with Medical Costs |
Other (explain) |
|
(Check all that apply) |
Food Stamp Assistance |
Help with Cost of Nursing Home, Rest Home or |
||
|
|
Home Care |
rn No |
|
Do you or any other household member receive assistance now? |
rn Yes |
If Yes, from which program(s)? List ID numbers. |
||
Do you need a reasonable accommodation or special help, because of a disability, in order to complete your What language do you speak best?
application?YesNo What type of special help do you need?
NAME AND ADDRESS
First Name |
|
M.I. |
Last Name |
|
Maiden Name |
|
Telephone Number |
|
|
|
|
|
|
|
|
Your # |
|
|
|
|
|
|
|
|
MESSAGE # |
|
Where do you live? |
Number |
Street |
|
Apt. Number |
Floor Number |
City |
State |
Zip Code |
Where is your mail sent if |
Number |
Street |
|
Apt. Number |
Floor Number |
City |
State |
Zip Code |
different from above? |
|
|
|
|
|
|
|
|
Previous Addresses
If you have lived here less than 36 months, list your previous addresses in that time.
|
|
|
|
|
|
|
|
Dates |
|
Was this home owned by |
|
Address (Street, City, State, Zip Code) |
|
|
|
|
|
From |
To |
a household member? |
|||
1 |
|
|
|
|
|
|
|
|
|
Yes |
No |
2 |
|
|
|
|
|
|
|
|
|
Yes |
No |
AUTHORIZED REPRESENTATIVE |
|
|
|
|
|
|
|
|
|
||
Do you wish t o appoint an Authorized Representative t o act o n your behalf? |
Yes |
No |
Are you making this application as a representative |
||||||||
for someone else? |
rn Yes |
No |
If you answered Yes t o either question, complete the section below. |
|
|
|
|||||
Type of Representatwe: |
|
rn HospitalIMedical Substance Abuse Treatment Facility |
|
Representative's Name |
|
|
|||||
Authorized Representative |
IJ Conservator |
rn Guardian |
rn |
Power of Attorney |
|
|
|
|
|||
Address (Street, City, State, Zip Code) |
|
|
|
|
|
|
|
Telephone Number |
|
||
ESTA FORMA ESTA DlSPONlBLE EN ESPANOL. PUEDE OBTENER UNA FORMA, LLAMANDO SU TRABAJADOR(A)
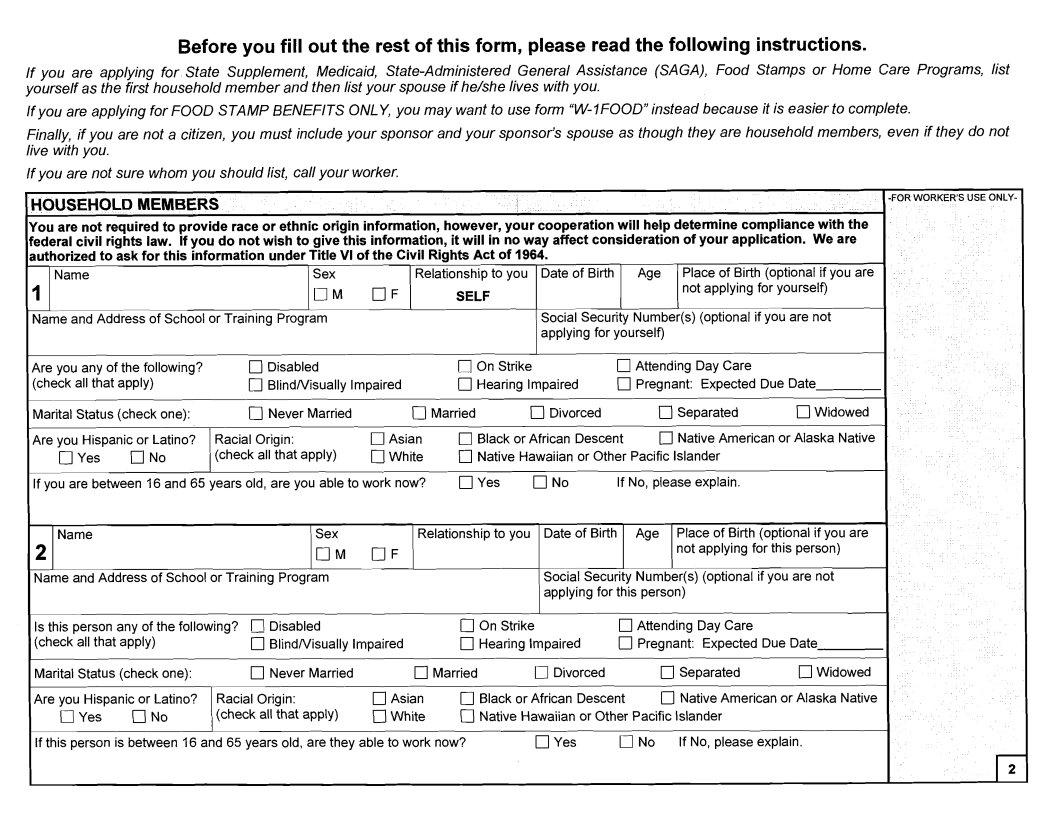
Before you fill out the rest of this form, please read the following instructions.
If you are applying for State Supplement, Medicaid,
If you are applying for FOOD STAMP BENEFITS ONLY, you may want to use form
Finally, if you are not a citizen, you must include your sponsor and your sponsor's spouse as though they are household members, even if they do not live with you.
If you are not sure whom you should list, call your worker.
HOUSEHOLD MEMBERS
You are not required to provide race or ethnic origin information, however, your cooperation will help determine compliance with the federal civil rights law. If you do not wish to give this information, it will in no way affect consideration of your application. We are authorized to ask for this information under Title VI of the Civil Rights Act of 1964.
Name |
Sex |
|
Relationship to you Date of Birth Age Place of Birth (optional if you are |
|
1 |
O M |
OF |
SELF |
not applying for yourself) |
|
||||
Name and Address of School or Training Program |
|
|
Social Security Number(s) (optional if you are not |
|
|
|
|
|
applying for yourself) |
Are you any of the following? |
q Disabled |
|
On Strike |
|
|
Attending Day Care |
|
|
(check all that apply) |
BlindNisually Impaired |
q Hearing Impaired |
q Pregnant: Expected Due Date |
|||||
Marital Status (check one): |
Never Married |
|
Married |
Divorced |
|
q Separated |
qWidowed |
|
Are you Hispanic or Latino? |
Racial Origin: |
Asian |
Black or African Descent |
Native American or Alaska Native |
||||
Yes |
No |
(check all that apply) |
White |
Native Hawaiian or Other Pacific Islander |
|
|||
If you are between 16 and 65 years old, are you able to work now? |
q Yes |
q No |
If No, please explain. |
|
||||
Name |
Sex |
2 |
O M OF |
Name and Address of School or Training Program |
|
Is this person any of the following? |
Disabled |
(check all that apply) |
q BlindNisually Impaired |
Relationship to you Date of Birth Age Place of Birth (optional if you are not applying for this person)
Social Security Number(s) (optional if you are not applying for this person)
On Strike |
q Attending Day Care |
q Hearing Impaired |
q Pregnant: Expected Due Date |
Marital Status (check one): |
q Never Married |
|
Are you Hispanic or Latino? |
Racial Origin: |
|
Yes |
q No |
(check all that apply) |
q Married |
q Divorced |
Separated |
Widowed |
q Asian |
Black or African Descent |
0 Native American or Alaska Native |
|
AWhite |
Native Hawaiian or Other Pacific Islander |
|
|
If this person is between 16 and 65 years old, are they able to work now? |
q Yes |
No |
If No, please explain. |
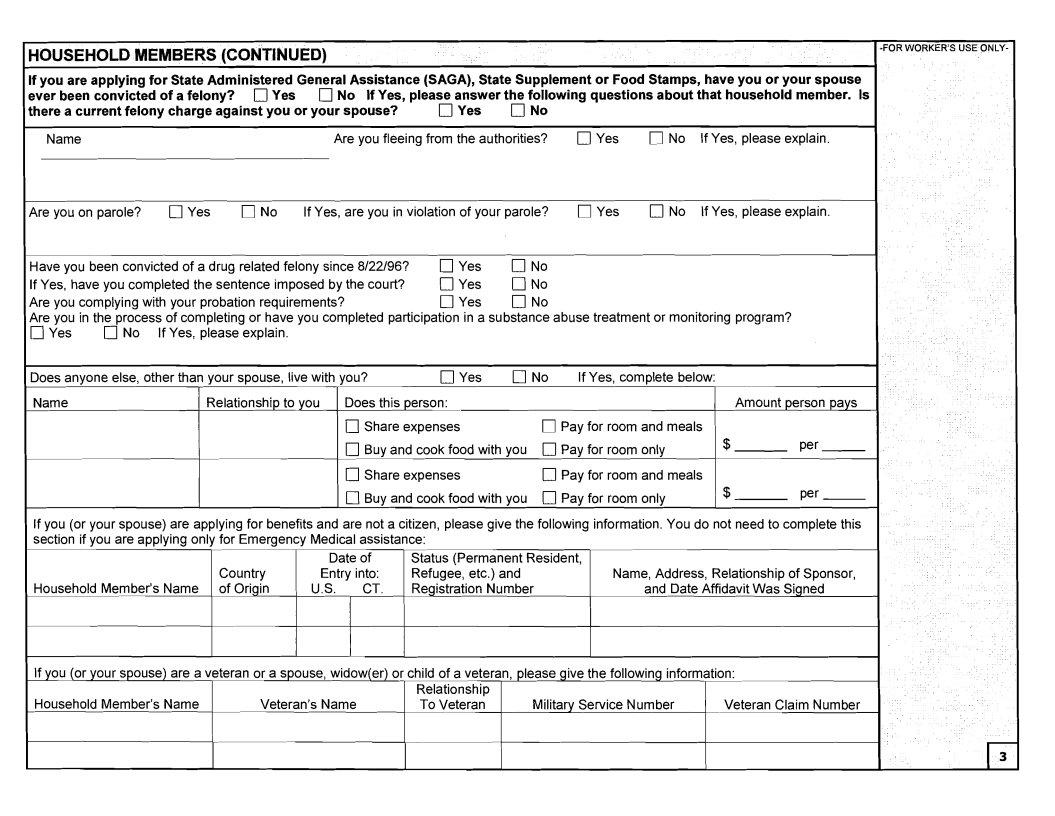
HOUSEHOLD MEMBERS (CONTINUED)
If you are applying for State Administered General Assistance (SAGA), State Supplement or Food Stamps, have you or your spouse
ever been convicted of a felony? |
Yes [7 No If Yes, please answer the following questions about that household member. Is |
||||
there a current felony charge against you or your spouse? |
Yes |
No |
|
|
|
Name |
Are you fleeing from the authorities? |
Yes |
0No If Yes, please explain. |
||
Are you on parole? |
Yes |
No |
If Yes, are you in violation of your parole? |
Yes |
No |
If Yes, please explain. |
|||||
Have you been convicted of a drug related felony since 8/22/96? |
[7 Yes |
No |
|
|
|
|
|||||
If Yes, have you completed the sentence imposed by the court? |
Yes |
No |
|
|
|
|
|||||
Are you complying with your probation requirements? |
|
Yes |
No |
|
|
|
|
||||
Are you in the process of completing or have you completed participation in a substance abuse treatment or monitoring program? |
|||||||||||
[7 Yes |
No |
If Yes, please explain. |
|
|
|
|
|
|
|
|
|
Does anyone else, other than your spouse, live with you? |
Yes |
No |
If Yes, complete below: |
|
|||||||
Name |
|
Relationship to you |
Does this person: |
|
|
|
|
Amount person pays |
|||
|
|
|
|
|
[7 Share expenses |
|
Pay for room and meals |
|
|||
|
|
|
|
|
[7 Buy and cook food with you |
|
Pay for room only |
|
$ |
Per - |
|
|
|
|
|
|
Share expenses |
|
Pay for room and meals |
|
|||
|
|
|
|
|
Buy and cook food with you |
|
Pay for room only |
|
$ |
Per - |
|
If you (or your spouse) are applying for benefits and are not a citizen, please give the following information. You do not need to complete this section if you are applying only for Emergency Medical assistance:
|
Date of |
Status (Permanent Resident, |
|
|
Country |
Entry into: |
Refugee, etc.) and |
Name, Address, Relationship of Sponsor, |
|
Household Member's Name of Origin |
U.S. |
CT. |
Registration Number |
and Date Affidavit Was Signed |
If you (or your spouse) are a veteran or a spouse, widow(er) or child of a veteran, please give the following information:
|
|
Relationship |
|
|
Household Member's Name |
Veteran's Name |
To Veteran |
Military Service Number |
Veteran Claim Number |
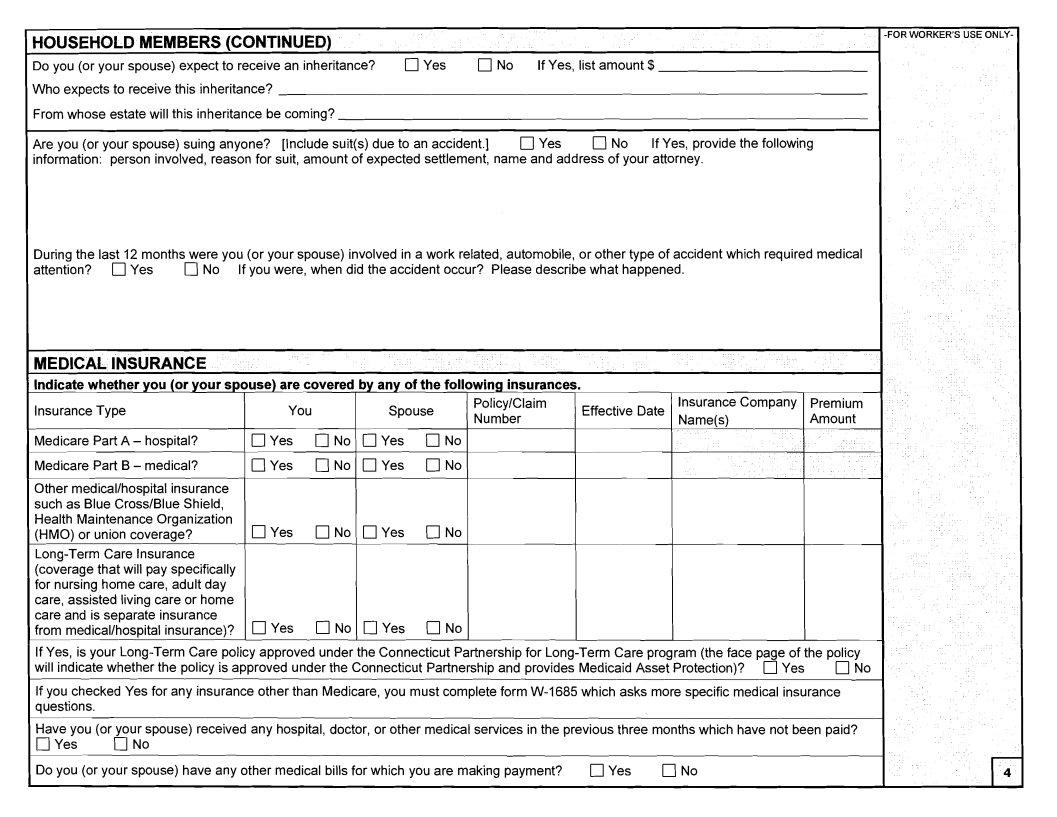
HOUSEHOLD MEMBERS (CONTINUED)
Do you (or your spouse) expect to receive an inheritance? |
Yes |
No |
If Yes, list amount $ |
Who expects to receive this inheritance?
From whose estate will this inheritance be coming?
Are you (or your spouse) suing anyone? [Include suit(s) due to an accident.]YesNo If Yes, provide the following information: person involved, reason for suit, amount of expected settlement, name and address of your attorney.
During the last 12 months were you (or your spouse) involved in a work related, automobile, or other type of accident which required medical
attention? |
Yes |
No If you were, when did the accident occur? Please describe what happened. |
MEDICAL INSURANCE
Indicate whether you (or your spouse) are covered by any of the following insurances.
Insurance Type
Medicare Part A - hospital?
Medicare Part B - medical?
Other medicallhospital insurance such as Blue CrossIBlue Shield, Health Maintenance Organization (HMO) or union coverage?
You |
|
Spouse |
Policy1C1airn |
Effective Date |
Insurance Company |
Premium |
|
|
Number |
Name(s) |
Amount |
||||
|
|
|
|
|
|||
Yes |
No |
El Yes |
El No |
|
|
|
|
Yes |
No |
El Yes |
No |
|
|
|
|
El Yes |
El No |
El Yes |
El No |
|
|
|
|
Yes No Yes No
If Yes, is your
will indicate whether the policy is approved under the Connecticut Partnership and provides Medicaid Asset Protection)? |
Yes |
No |
If you checked Yes for any insurance other than Medicare, you must complete form
Have you (or your spouse) received any hospital, doctor, or other medical services in the previous three months which have not been paid?
YesNo
Do you (or your spouse) have any other medical bills for which you are making payment? |
Yes |
No |
LEGALLY LIABLE RELATIVE INFORMATION
List your parents if you are not living with them and you are under age 18.
|
|
|
Date parent |
Do you receive money |
|
Absent Parent's Name |
Child(ren)'s Name(s) |
Parent's Address |
left home |
from this person? |
|
- |
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
IJYes |
IJNo |
If you are married and your spouse is not living with you, complete the following items: |
|
|
|
||
Spouse Name |
Address |
|
|
Date of Separation |
|
ASSETS
Tell us about the assets owned by you (or your spouse). Also, tell us about any asset with your name (or the name of your spouse) even if the asset is not yours. Answer each numbered section. Complete any section where you answered Yes.
1. CASH ON HAND (Money that is not in an account) |
Yes |
No |
|
||
Name |
|
Amount |
|
Name |
Amount |
|
$ |
|
|
|
$ |
2. BANKICREDIT UNION ACCOUNTS |
Yes |
No |
List savings, checking, C.D., I.R.A., vacation, Christmas club, burial |
||
accounts or any other type of account. Include joint and trustee accounts listed under your name (or the name of your spouse), even if the money is not yours or theirs. Also, include accounts, such as those for children, held in trust for you (or your spouse).
Name |
BankICredit Union Name and Address |
Account Number |
Balance |
|
|
|
$ |
- |
I |
$
-
$
$
3. LIFE INSURANCE POLlClESlDEATH BENEFITS (Include group policies) |
[7 Yes |
No |
|
Company Name and Address |
|
Policy Number |
Face Value |
|
|
|
$ |
$

ASSETS (CONTINUED)
4. |
ANNUlTlESrrRUST FUNDSILIMITED PARTNERSHIPS |
Yes |
No |
|
|||
|
Name |
Company Name and Address |
|
Account Number |
Amount |
||
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
$ |
5. |
STOCKSIMUTUAL FUNDSlBONDS1U.S. SAVINGS BONDS |
Yes |
No For stocks and mutual funds, identify owner, name |
||||
|
of company, number of shares and value. For bonds, identify owner, type of bond, serial number, date of purchase and denomination. |
||||||
6. |
PREPAID FUNERAL CONTRACT |
Yes |
No |
|
|
|
|
|
Name |
Funeral Home Name and Address |
|
|
Amount |
||
|
|
|
|
|
|
|
$ |
Motor Vehicles I
Do you (or your spouse) own, have registered or have listed in yourltheir name a car, truck, boat, camper, recreational vehicle, trailer,
motorcycle or other vehicle (include unregistered vehicles)? |
Yes |
No |
If Yes, complete the following section: |
||||
|
Vehicle |
|
|
|
|
License Plate |
|
Owner Name |
Type |
Year |
Make |
Model |
Mileage |
Number |
Amount Owed |
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
$ |
Real Estate I
Do you (or your spouse) own any real estate (include home, land, and
Owner(s) |
Location (Street, Town, State) |
1
lfyou are applying for
Yes No
Is this: |
[7 land only |
[7 single family dwelling |
other (specify |
1 |
||
Owner(s) |
Location (Street, Town, State) |
|
|
|||
2 |
|
|
|
|
|
|
Is this: |
[7 land only |
single family dwelling |
[7 other (specify |
1 |
||
Do you (or your spouse) have |
Yes |
No |
|
|
||
Other Assets I
Do you (or your spouse) own any other assets not listed above (for example, contents of safe deposit box, mortgage payable to you, jewelry,
furs, paintings, etc.)? |
[7 Yes |
[7 No If Yes, identify owner, asset and value. |
Transfer of Assets I
Have you (or your spouse) sold, traded, given away, or transferred ownership of any motor vehicles, bank accounts, property of any kind,
stocks, bonds, mutual funds or cash during the last |
Yes |
No |
Have you had assets transferred through the probate court/surrogate courts in state or out of state in the last 36 months? |
Yes |
[7 No |
If Yes to either question, what was transferred, sold or given away, to whom, when, and how much money or what was received in return? (Attach an additional page if needed.)
Have you (or your spouse) established a trust or funded a trust with income or property of any kind within the past 60 months?
Yes No If Yes, provide additional details. (Attach an additional page if needed.)
Have you (or your spouse) closed any type of account during the last
Yes |
No If Yes, explain below. Include the bank name, address, account number and date closed. |
Have you (or your spouse) sold or junked a motor vehicle in the last
Yes No
INCOME
How have you paid your bills during the last six months? If you have no income or your expenses are greater than your income, how do you pay your bills?
Current and Previous Employment Income I
Are you (or your spouse) employed
Is anyone
sell homemade crafts, clean house, etc.?Yes No
If you answered Yes to either of the above two questions, complete the following section. If a person has more than one job, list each job separately. Include anyone who receives income from a job training program.
If No, list the last job held by each person within the last year. Attach an additional page if needed.
Name |
Pay before deductions |
Tips? |
Yes |
No |
Hours worked |
Date Started |
Date Ended |
|
1 |
$ |
Per |
Weekly amount $ |
|
per week |
|
|
|
|
|
|
|
|
||||
Employer Name and Address |
|
|
|
|
|
Reason For Leaving |
|
|
Name |
Pay before deductions |
Tips? |
Yes |
No |
Hours worked |
Date Started |
Date Ended |
|
2 |
$ |
Per |
Weekly amount $ |
|
per week |
|
|
|
|
|
|
|
|
||||
Employer Name and Address |
|
|
|
|
|
Reason For Leaving |
|
|
Current and Previous Employment Income (continued) I
Have you (or your spouse) quit or been fired from a job in the last ninety days? |
Yes |
No |
If Yes, list name(s) and reason(s) for |
|
quitting or being fired. |
|
|
|
|
Name |
Name of Former Employer |
|
Reason for Quit or Fire |
|
Dependent Care I
Do you (or your spouse) pay someone for day care for a child or disabled adult so that you, he or she can work, attend training or
look for a job? |
Yes |
No If Yes, complete below: |
|
|
||
Name (Who day care is for) |
Amount Per Week |
Name and Address of Day Care Provider |
Telephone Number |
|||
|
|
$ |
|
|
|
|
|
|
$ |
|
|
|
|
Does the State or anyone else pay your day care? |
Yes |
No If Yes, how much? |
Amount $ |
|
||
Students |
I |
|
|
|
|
|
|
|
|
|
|
|
|
Are there any students |
Yes |
No |
||||
If Yes, complete the following section. |
|
|
|
|
||
Name of Student |
|
School or Program |
|
|
|
|
|
|
|
|
|
|
- |
Expected Date of Graduation |
Semester Hours |
Tuition & Mandatory Fees |
|
|
||
|
|
|
$ |
|
|
|
Is this student on a meal plan? |
Yes |
No |
Does this student have a job? |
Yes |
No |
Does this student receive federally funded
If Yes, how many hours per week?
Yes |
No If Yes, how many hours each week? |
Does this student receive any educational grants, loans, and scholarships, including |
Yes |
No |
If Yes, form |
|
|
Other Income 1
Check Yes or No to indicate if you (or your spouse) receive or have applied for money from any of the following sources:
1) |
Child Support andlor Alimony |
O Y e s |
O N o |
5) |
Other Government Benefits (Types are: Railroad Retirement, |
||
|
|
|
|
|
Educational Loans and Grants, Veterans Benefits, VA Aid |
||
2) |
Social Security [Types are: |
|
|
|
and Attendance, Military Allotment and HUD Subsidy) |
|
|
|
Retirement (OA), Disability, Survivor's |
|
|
|
|
O Y e s |
O N o |
|
Disability Insurance (SDI) |
Yes |
No |
|
|
|
|
|
|
q Yes |
|
6) Other Private Benefits: MaternitylSick Pay, Pensions, |
q No |
||
3) SSI (Supplemental Security Income) |
No |
|
Worker's Compensation, Union Benefits |
q Yes |
|||
4) |
Unemployment Compensation |
Yes |
q No |
7) |
Other Income: from Stocks, Bonds, Annuities, Rental |
|
|
|
|
|
|
|
Property, Roomers, Boarders, Money from Friends or |
|
|
|
|
|
|
|
Relatives, Any Other Source |
O Y e s |
O N o |
If you (or your spouse) are receiving income from any of the sources listed above, complete the following:
|
|
Amount Receiving1 |
IDlClaim Number(s) (Optional |
Name |
Type of Income |
How Often? |
if not applying for assistance) |
|
$ |
per |
|
|
$ |
per |
|
|
$ |
per |
|
|
$ |
per |
|
If you (or your spouse) have applied for income from any of the sources listed above, complete the following:
Name |
Type of Income |
Date of Application or Claim |
Have you (or your spouse) received cash assistance for your family from any state or U.S. territory other than Connecticut since 1011196?
q Yes q No If Yes, from which state or U.S. territory? |
When? From |
|
To |
|
|
Have you (or your spouse) received any other assistance from another state within the last 90 days? |
q Yes |
q No |
If Yes, |
||
which type of assistance? q Food Stamps |
Medical |
From which State? |
|
|
|
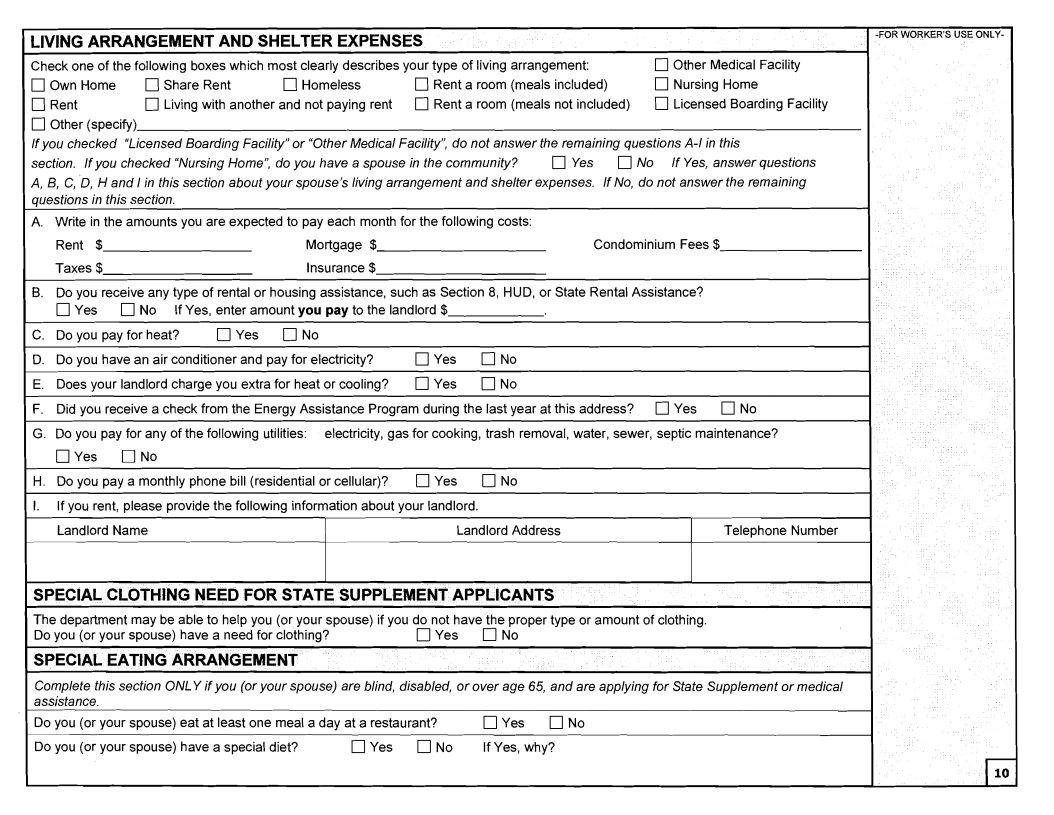
LIVING ARRANGEMENT AND SHELTER EXPENSES
Check one of the following boxes which most clearly describes your type of living arrangement: |
q Other Medical Facility |
|||
q Own Home |
q Share Rent |
q Homeless |
q Rent a room (meals included) |
q Nursing Home |
q Rent |
q Living with another and not paying rent |
q Rent a room (meals not included) |
q Licensed Boarding Facility |
|
q Other (specify)
I f you checked "Licensed Boarding Facility" or "Other Medical Facility", do not answer the remaining questions
section. I f you checked "Nursing Home", do you have a spouse in the community? q Yes q No I f Yes, answer questions A, B, C, D, H and Iin this section about your spouse's living arrangement and shelter expenses. I f No, do not answer the remaining
questions in this section. |
|
|
A. Write in the amounts you are expected to pay each month for the following costs: |
|
|
Rent $ |
Mortgage $ |
Condominium Fees $ |
Taxes $ |
Insurance $ |
|
B.Do you receive any type of rental or housing assistance, such as Section 8, HUD, or State Rental Assistance? q Yes q No If Yes, enter amount you pay to the landlord $
C. |
Do you pay for heat? |
q Yes |
q No |
|
|
|
D. |
Do you have an air conditioner and pay for electricity? |
q Yes |
q No |
|
||
E. |
Does your landlord charge you extra for heat or cooling? |
q Yes |
q No |
|
||
F. |
Did you receive a check from the Energy Assistance Program during the last year at this address? q Yes |
q No |
||||
G. Do you pay for any of the following utilities: electricity, gas for cooking, trash removal, water, sewer, septic maintenance?
q Yes I7 No |
|
H. Do you pay a monthly phone bill (residential or cellular)? |
q Yes q No |
I.If you rent, please provide the following information about your landlord.
Landlord NameLandlord AddressTelephone Number
SPECIAL CLOTHING NEED FOR STATE SUPPLEMENT APPLICANTS
The department may be able to help you (or your spouse) if you do not have the proper type or amount of clothing.
Do you (or your spouse) have a need for clothing?q Yes q No
SPECIAL EATING ARRANGEMENT
Complete this section ONLY if you (or your spouse) are blind, disabled, or over age 65, and are applying for State Supplement or medical assistance.
Do you (or your spouse) eat at least one meal a day at a restaurant? |
O Y e s O N o |
|
Do you (or your spouse) have a special diet? |
q Yes q No |
If Yes, why? |

CHILD SUPPORT DEDUCTION- FOOD STAMP PROGRAM |
||
|
||
Do you (or your spouse) pay court ordered child support to someone for a child(ren) who is not a member of your household? |
|
|
Yes |
No If Yes, complete one of the following sections for each person to whom you pay child support. |
|
Name and address of the person you send the child support payments to: (If you make payments to a state, list the state and file number)
Name and date of birth of the child(ren) for whom you pay this child support: |
|
|
|
Name |
DOB |
Name |
DOB |
What is the amount of child support that has been ordered by the court? $
How much child support do you actually pay each month? $
How often is support due?
Do you pay by wage withholding? |
Yes |
No |
Have you been paying child support for three or more months within the last |
Yes |
No |
||||
Are your support payments up to date? |
Yes |
No |
|
|
|
|
Are you making payments to reduce an arrearage (back support)? |
Yes |
No |
|
|
||
If yes, how much do you pay on the arrearage? |
$ |
|
How often do you pay? |
|
||
READ CAREFULLY AND SIGN
FOR ALL PROGRAMS
I understand and agree to the following:
I will notify the Department of Social Services within 10 days of any change in income, assets or living arrangements.
I may request a hearing in writing if I disagree with an action taken on my case. I may request a hearing orally if applying for Food Stamps.
All information given on this form is subject to verification by federal, state and local officials. I will cooperate with these officials by providing authorizations, documents and other proof to prove what I have said. I authorize the Department of Social Services to verify any information given on this form.
If I make a false or misleading statement, I may be referred for prosecution.
All information given on this form, including Social Security numbers, is confidential, except as authorized or required by state or federal law, and will be used only to administer all programs except for certain exceptions for the Food Stamp and SAGA programs indicated below. Information I give on this form may be shared with law enforcement officials in order to locate and arrest persons fleeing to avoid the law.
I give my permission to the department to release information about me and others in my family who are receiving benefits for purposes directly connected with the administration of the department's programs. Purposes directly connected with the administration of the department's programs include, but are not limited to, establishing eligibility, determining the amount of assistance, providing services, and the investigation, prosecution, or civil proceedings related to the administration of the department's programs.
I declare that I and the other people for whom I am requesting benefits are either United States citizens or, in the event any of us are not, that the information I have provided regarding anyone's
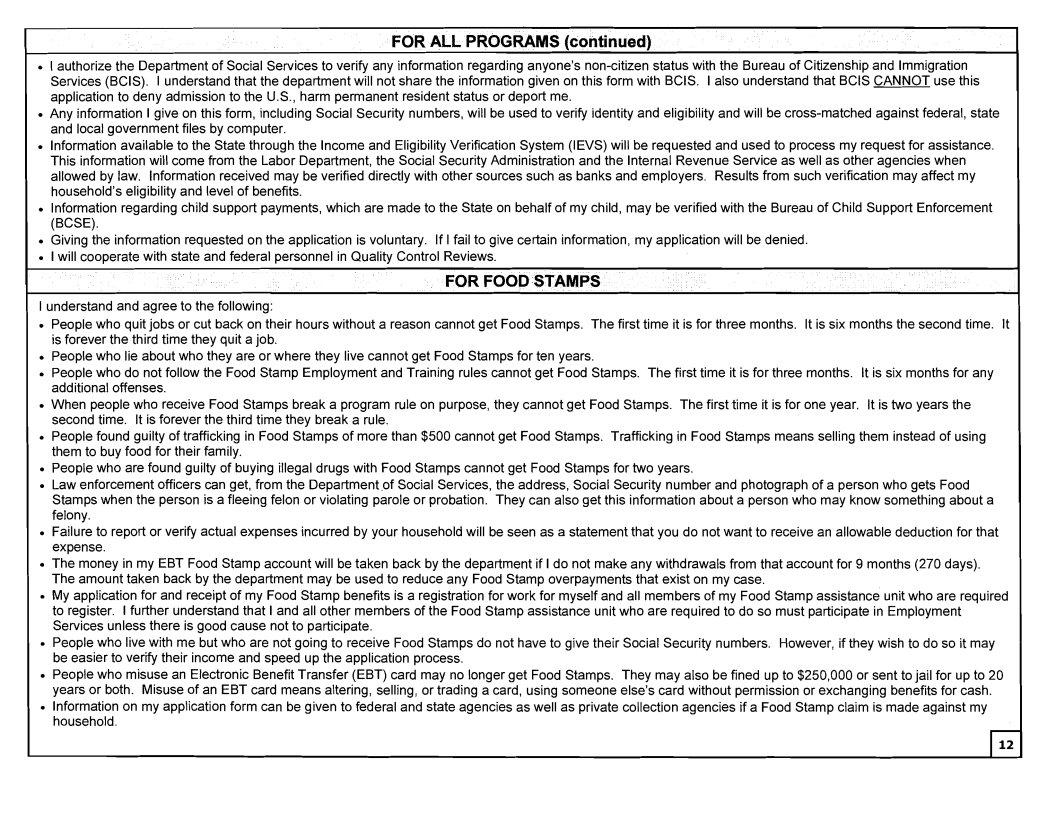
FOR ALL PROGRAMS (continued)
I authorize the Department of Social Services to verify any information regarding anyone's
Any information I give on this form, including Social Security numbers, will be used to verify identity and eligibility and will be
lnformation available to the State through the Income and Eligibility Verification System (IEVS) will be requested and used to process my request for assistance. This information will come from the Labor Department, the Social Security Administration and the Internal Revenue Service as well as other agencies when allowed by law. lnformation received may be verified directly with other sources such as banks and employers. Results from such verification may affect my household's eligibility and level of benefits.
lnformation regarding child support payments, which are made to the State on behalf of my child, may be verified with the Bureau of Child Support Enforcement (BCSE).
Giving the information requested on the application is voluntary. If I fail to give certain information, my application will be denied. I will cooperate with state and federal personnel in Quality Control Reviews.
FOR FOOD STAMPS
.I understand and agree to the following:
People who quit jobs or cut back on their hours without a reason cannot get Food Stamps. The first time it is for three months. It is six months the second time. It is forever the third time they quit a job.
People who lie about who they are or where they live cannot get Food Stamps for ten years.
People who do not follow the Food Stamp Employment and Training rules cannot get Food Stamps. The first time it is for three months. It is six months for any additional offenses.
When people who receive Food Stamps break a program rule on purpose, they cannot get Food Stamps. The first time it is for one year. It is two years the second time. It is forever the third time they break a rule.
People found guilty of trafficking in Food Stamps of more than $500 cannot get Food Stamps. Trafficking in Food Stamps means selling them instead of using them to buy food for their family.
People who are found guilty of buying illegal drugs with Food Stamps cannot get Food Stamps for two years.
Law enforcement officers can get, from the Department of Social Services, the address, Social Security number and photograph of a person who gets Food Stamps when the person is a fleeing felon or violating parole or probation. They can also get this information about a person who may know something about a felony.
Failure to report or verify actual expenses incurred by your household will be seen as a statement that you do not want to receive an allowable deduction for that expense.
The money in my EBT Food Stamp account will be taken back by the department if I do not make any withdrawals from that account for 9 months (270 days). The amount taken back by the department may be used to reduce any Food Stamp overpayments that exist on my case.
My application for and receipt of my Food Stamp benefits is a registration for work for myself and all members of my Food Stamp assistance unit who are required to register. I further understand that I and all other members of the Food Stamp assistance unit who are required to do so must participate in Employment Services unless there is good cause not to participate.
People who live with me but who are not going to receive Food Stamps do not have to give their Social Security numbers. However, if they wish to do so it may be easier to verify their income and speed up the application process.
People who misuse an Electronic Benefit Transfer (EBT) card may no longer get Food Stamps. They may also be fined up to $250,000 or sent to jail for up to 20 years or both. Misuse of an EBT card means altering, selling, or trading a card, using someone else's card without permission or exchanging benefits for cash. lnformation on my application form can be given to federal and state agencies as well as private collection agencies if a Food Stamp claim is made against my household.
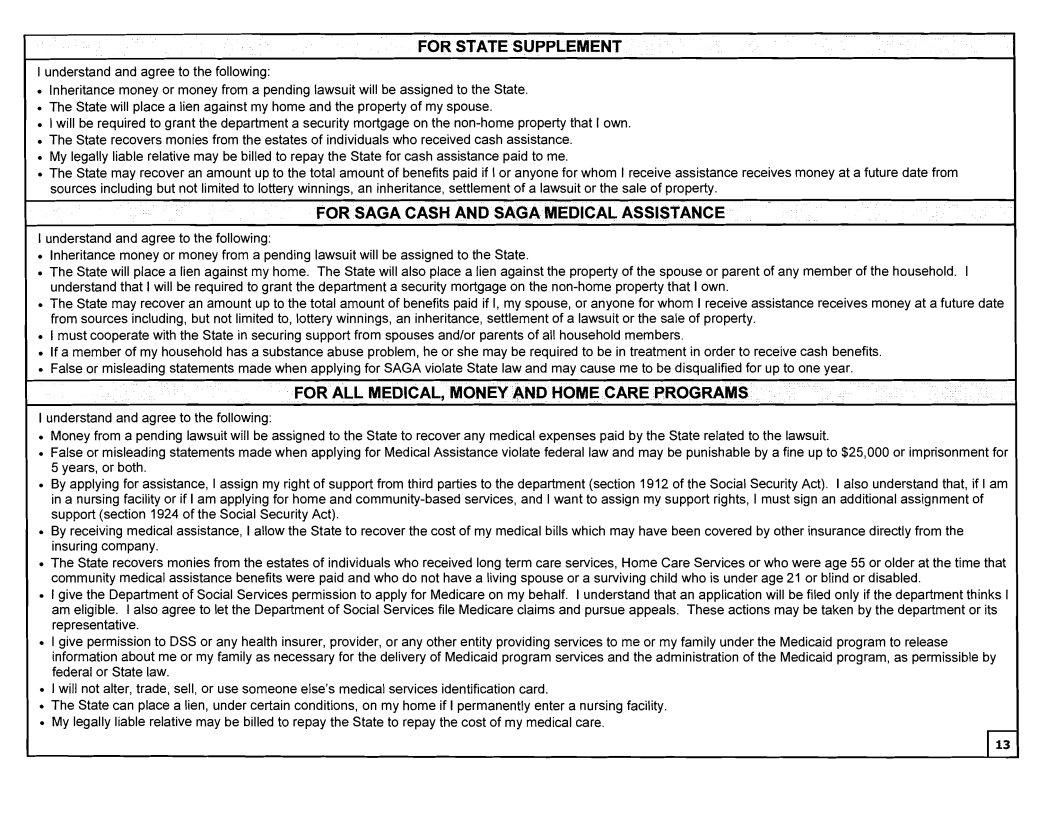
FOR STATE SUPPLEMENT
I understand and agree to the following:
lnheritance money or money from a pending lawsuit will be assigned to the State. The State will place a lien against my home and the property of my spouse.
I will be required to grant the department a security mortgage on the
My legally liable relative may be billed to repay the State for cash assistance paid to me.
The State may recover an amount up to the total amount of benefits paid if I or anyone for whom I receive assistance receives money at a future date from sources including but not limited to lottery winnings, an inheritance, settlement of a lawsuit or the sale of property.
FOR SAGA CASH AND SAGA MEDICAL ASSISTANCE
I understand and agree to the following:
lnheritance money or money from a pending lawsuit will be assigned to the State.
The State will place a lien against my home. The State will also place a lien against the property of the spouse or parent of any member of the household. I understand that I will be required to grant the department a security mortgage on the
The State may recover an amount up to the total amount of benefits paid if I, my spouse, or anyone for whom I receive assistance receives money at a future date from sources including, but not limited to, lottery winnings, an inheritance, settlement of a lawsuit or the sale of property.
I must cooperate with the State in securing support from spouses and/or parents of all household members.
If a member of my household has a substance abuse problem, he or she may be required to be in treatment in order to receive cash benefits. False or misleading statements made when applying for SAGA violate State law and may cause me to be disqualified for up to one year.
FOR ALL MEDICAL, MONEY AND HOME CARE PROGRAMS
I understand and agree to the following:
Money from a pending lawsuit will be assigned to the State to recover any medical expenses paid by the State related to the lawsuit.
False or misleading statements made when applying for Medical Assistance violate federal law and may be punishable by a fine up to $25,000 or imprisonment for 5 years, or both.
By applying for assistance, I assign my right of support from third parties to the department (section 1912 of the Social Security Act). I also understand that, if I am in a nursing facility or if I am applying for home and
By receiving medical assistance, I allow the State to recover the cost of my medical bills which may have been covered by other insurance directly from the insuring company.
The State recovers monies from the estates of individuals who received long term care services, Home Care Services or who were age 55 or older at the time that community medical assistance benefits were paid and who do not have a living spouse or a surviving child who is under age 21 or blind or disabled.
I give the Department of Social Services permission to apply for Medicare on my behalf. I understand that an application will be filed only if the department thinks I am eligible. I also agree to let the Department of Social Services file Medicare claims and pursue appeals. These actions may be taken by the department or its representative.
I give permission to DSS or any health insurer, provider, or any other entity providing services to me or my family under the Medicaid program to release information about me or my family as necessary for the delivery of Medicaid program services and the administration of the Medicaid program, as permissible by federal or State law.
I will not alter, trade, sell, or use someone else's medical services identification card.
The State can place a lien, under certain conditions, on my home if I permanently enter a nursing facility. My legally liable relative may be billed to repay the State to repay the cost of my medical care.

SIGNATURES
.I have read this form or have had it read to me in a language that I understand. I certify that the information given on this form is true and complete to the best of my knowledge. If I have knowingly given incorrect information, I may be subject to penalties for false statement as specified in the Connecticut General Statutes Section
X |
|
If someone helped the applicant complete this form, this person must sign also. |
||
Applicant's Signature |
Date |
|
|
|
Spouse's Signature |
Date |
Helper's Signature |
Relationship (if any) |
Date |
|
|
If someone completed this form on the recipient's behalf, this representative |
||
Witness' Signature (if signed with an X) |
Date |
must sign also. |
|
|
Interpreter's Signature |
Date |
Representative's Signature |
|
Date |
Printed Name of InterpreterlRepresentative |
Date |
Reviewed by |
|
Date |
AUTHORIZATION TO DISCLOSE APPLICATION STATUS
1, |
, hereby authorize the Department of Social Services to share information regarding the status of this application |
|
for assistance with the following individuals, agencies or institutions: |
|
|
Name |
Address |
Telephone Number |
Applicant's or Authorized Representative's Signature |
Date |
FOR HOSPITAL AND SUBSTANCE ABUSE TREATMENT FACILITY REPRESENTATIVES
I certify that the applicant was informed of hislher responsibility to complete this application; and that hislher signature could not be obtained for the following reason(s):
Your Right to Make a Discrimination Complaint: Under federal and state law you have the right to make a discrimination complaint if you think we have taken actions against you because of your race, color, religious creed, sex, marital status, age, national origin, ancestry, criminal record, political beliefs, sexual orientation, mental retardation, mental disability, learning disability or physical disability, including but not limited to blindness. You or someone representing you may write to or call one or more of these agencies to make a discrimination complaint: Commissioner of the Department of Social Services, Attention Affirmative Action Division DirectorlADA Coordinator, 25 Sigourney Street, Hartford, CT