
You could fill in FALSE effortlessly with the help of our PDFinity® online PDF tool. To make our editor better and more convenient to utilize, we continuously develop new features, with our users' feedback in mind. To get the process started, take these basic steps:
Step 1: First of all, access the pdf tool by pressing the "Get Form Button" above on this page.
Step 2: The editor helps you change the majority of PDF files in various ways. Enhance it with your own text, adjust what is already in the document, and place in a signature - all at your convenience!
When it comes to blank fields of this precise document, here's what you want to do:
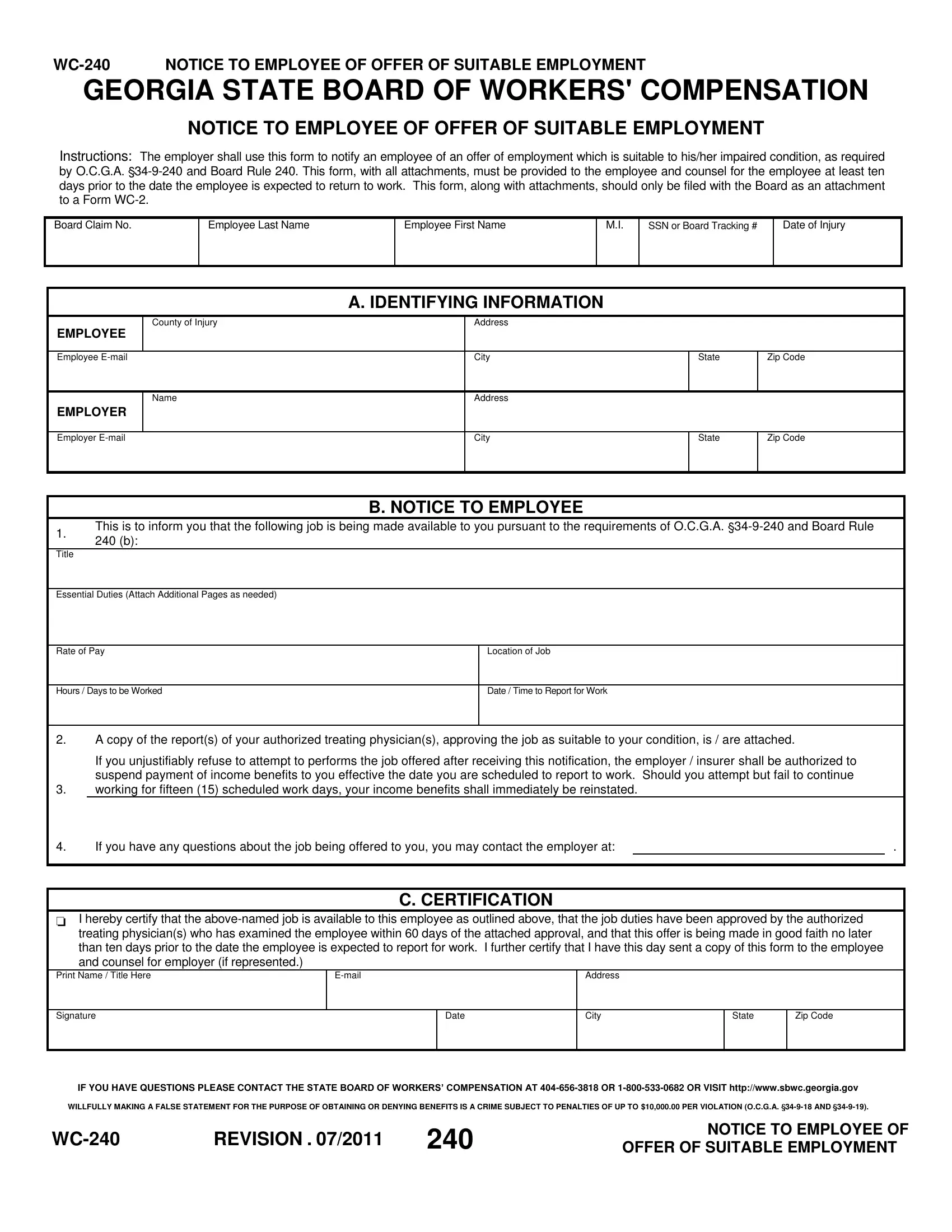
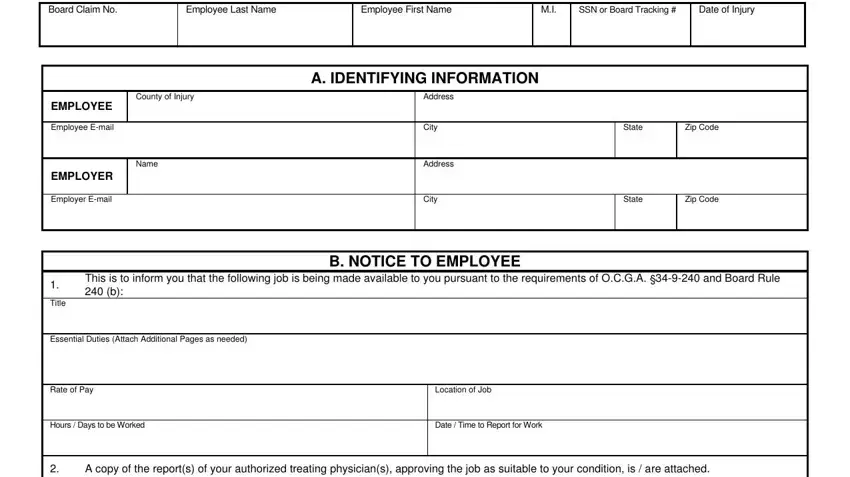
1. The FALSE involves particular information to be typed in. Ensure the following blanks are completed:
2. Once your current task is complete, take the next step – fill out all of these fields - If you have any questions about, I hereby certify that the, treating physicians who has, C CERTIFICATION, Email, Date, Address, City, State, Zip Code, IF YOU HAVE QUESTIONS PLEASE, WILLFULLY MAKING A FALSE STATEMENT, REVISION, NOTICE TO EMPLOYEE OF, and OFFER OF SUITABLE EMPLOYMENT with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
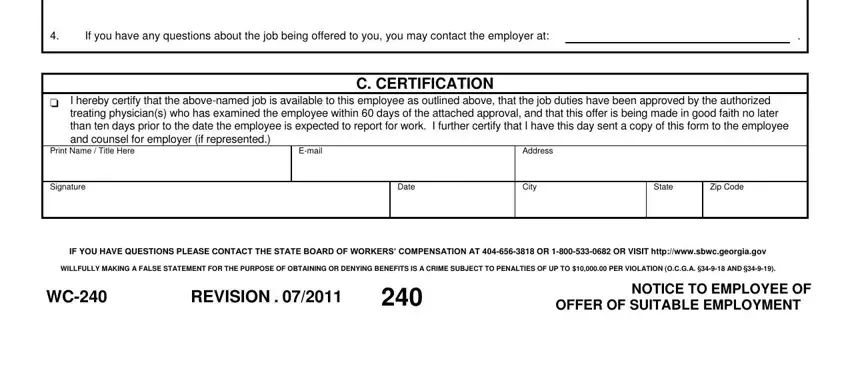
When it comes to Date and Address, ensure that you double-check them in this section. The two of these could be the key fields in this PDF.
Step 3: Immediately after taking another look at your form fields you've filled out, press "Done" and you are good to go! Right after registering a7-day free trial account at FormsPal, you will be able to download FALSE or email it immediately. The PDF will also be at your disposal via your personal account with your every single edit. FormsPal is committed to the personal privacy of all our users; we make sure that all personal data going through our editor is secure.