In the realm of worker's compensation in Georgia, the WC-R2 Rehabilitation Transmittal Form stands as a critical document, channeling essential information between injured employees, employers, rehabilitation providers, and the Georgia State Board of Workers' Compensation. By meticulously capturing details such as the employee's personal information, injury specifics, rehabilitation plan expectations, and progress reports, this form plays a pivotal role in ensuring a transparent and streamlined rehabilitation process. Designed to facilitate various types of reports, including those for catastrophic cases and standard medical care, it requires the attachment of pertinent documents like medical reports, job analyses, and vocational evaluations that underpin the rehabilitation efforts. Furthermore, the form emphasizes the procedural aspect, mandating a certificate of service for ensuring all involved parties receive the necessary documentation. Moreover, it outlines a clear procedure for approval or objection, signifying the steps to follow if disagreements arise, all while underscoring the legal ramifications of providing false information. This comprehensive approach not only aids in the effective management of workers' compensation claims but also underscores the shared responsibility among all parties to foster a fair and efficient path back to work for injured employees.
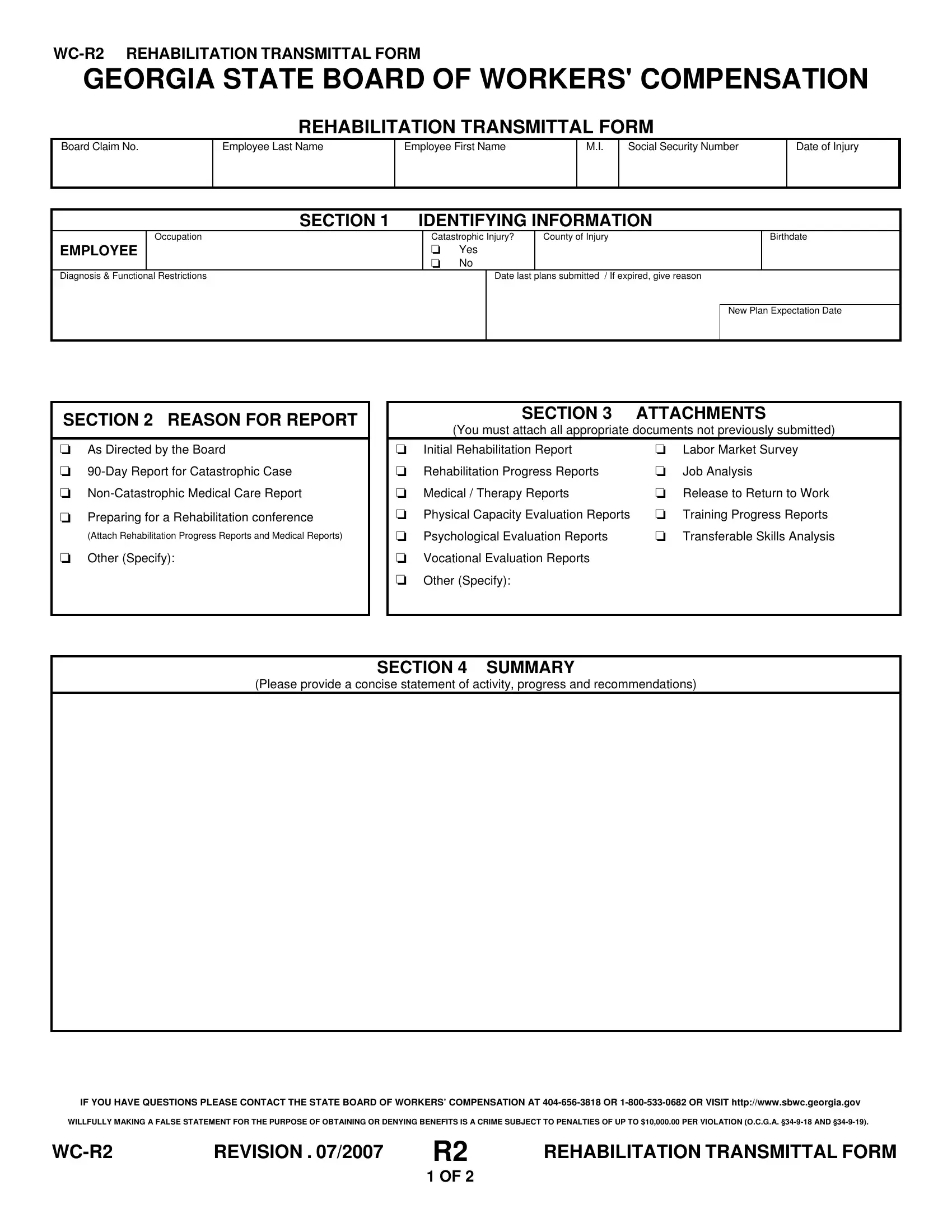
| Question | Answer |
|---|---|
| Form Name | Form Wc R2 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | wc r2 dbhdd wc 6 wage statement form |
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
REHABILITATION TRANSMITTAL FORM
Board Claim No.
Employee Last Name
Employee First Name
M.I.
Social Security Number
Date of Injury
|
SECTION 1 |
IDENTIFYING INFORMATION |
|
|
||||
|
Occupation |
|
Catastrophic Injury? |
County of Injury |
|
Birthdate |
||
EMPLOYEE |
|
|
0 |
Yes |
|
|
|
|
|
|
|
0 |
No |
|
|
|
|
Diagnosis & Functional Restrictions |
|
|
|
Date last plans submitted / If expired, give reason |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
New Plan Expectation Date |
|
|
|
|
|
|
|
|
|
|
SECTION 2 REASON FOR REPORT
0As Directed by the Board
0
0
0Preparing for a Rehabilitation conference
(Attach Rehabilitation Progress Reports and Medical Reports)
0Other (Specify):
SECTION 3 ATTACHMENTS
(You must attach all appropriate documents not previously submitted)
0 |
Initial Rehabilitation Report |
0 |
Labor Market Survey |
0 |
Rehabilitation Progress Reports |
0 |
Job Analysis |
0 |
Medical / Therapy Reports |
0 |
Release to Return to Work |
0 |
Physical Capacity Evaluation Reports |
0 |
Training Progress Reports |
0 |
Psychological Evaluation Reports |
0 |
Transferable Skills Analysis |
0Vocational Evaluation Reports
0Other (Specify):
SECTION 4 SUMMARY
(Please provide a concise statement of activity, progress and recommendations)
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2007 |
R2 |
REHABILITATION TRANSMITTAL FORM |
|
|
|
1 OF 2 |
|
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
SECTION 5 CERTIFICATE OF SERVICE
This section must be completed by the requesting party.
0 I certify that I have mailed copies to the following parties on |
|
|
/ |
|
|
/ |
|
|
at the current addresses below. |
|||||||||||
|
|
|
|
|
|
|
|
|
Month |
|
|
|
Day |
|
|
Year |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Signature |
|
|
|
|
|
|
|
|
|
|
Registration No. |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Rehabilitation Supplier Name |
|
|
Telephone |
|
|
|
|
Address |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
Zip Code |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Last Name |
|
First Name |
|
|
|
M.I. |
Address |
|
|
|
|
|
||||||
EMPLOYEE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Telephone Number |
|
|
|
|
City |
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Name |
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
||||
EMPLOYER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Telephone Number |
|
|
|
|
City |
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INSURER / |
|
Name |
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLAIMS OFFICE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Telephone Number |
|
|
|
|
City |
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
EMPLOYEE’S |
|
Name |
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
ATTORNEY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Telephone Number |
|
|
|
|
City |
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
EMPLOYER’S |
|
Name |
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
ATTORNEY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Telephone Number |
|
|
|
|
City |
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Name |
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|||
SITF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Telephone Number |
|
|
|
|
City |
|
|
State |
|
Zip Code |
||||||
|
|
|
|
|
|
|
||||||||||||||
Is this case applicable for Kid’s Chance scholarships? 0 Yes 0 No |
If yes, submit application to Kid’s Chance, Inc. |
|
||||||||||||||||||
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
SECTION 6 |
APPROVAL / OBJECTIONS, TWENTY (20) DAY NOTICE |
|
||||||||||||||
Absent written objections within 20 days of the date mailed, the rehabilitation request is approved effective the date of the certificate of service. No further correspondence will be issued by the Board. If there is an objection:
(1) The Objection must be in writing.
(2) It must be received by the Georgia State Board of Workers’ compensation within 20 days of the date of the Certificate of Service.
(3) A Certificate of Service must be completed stating that copies of the written objections were placed in the mail to all parties and the principal rehabilitation supplier the same date as the Certificate of Service.
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2007 |
R2 |
REHABILITATION TRANSMITTAL FORM |
|
|
|
2 OF 2 |
|