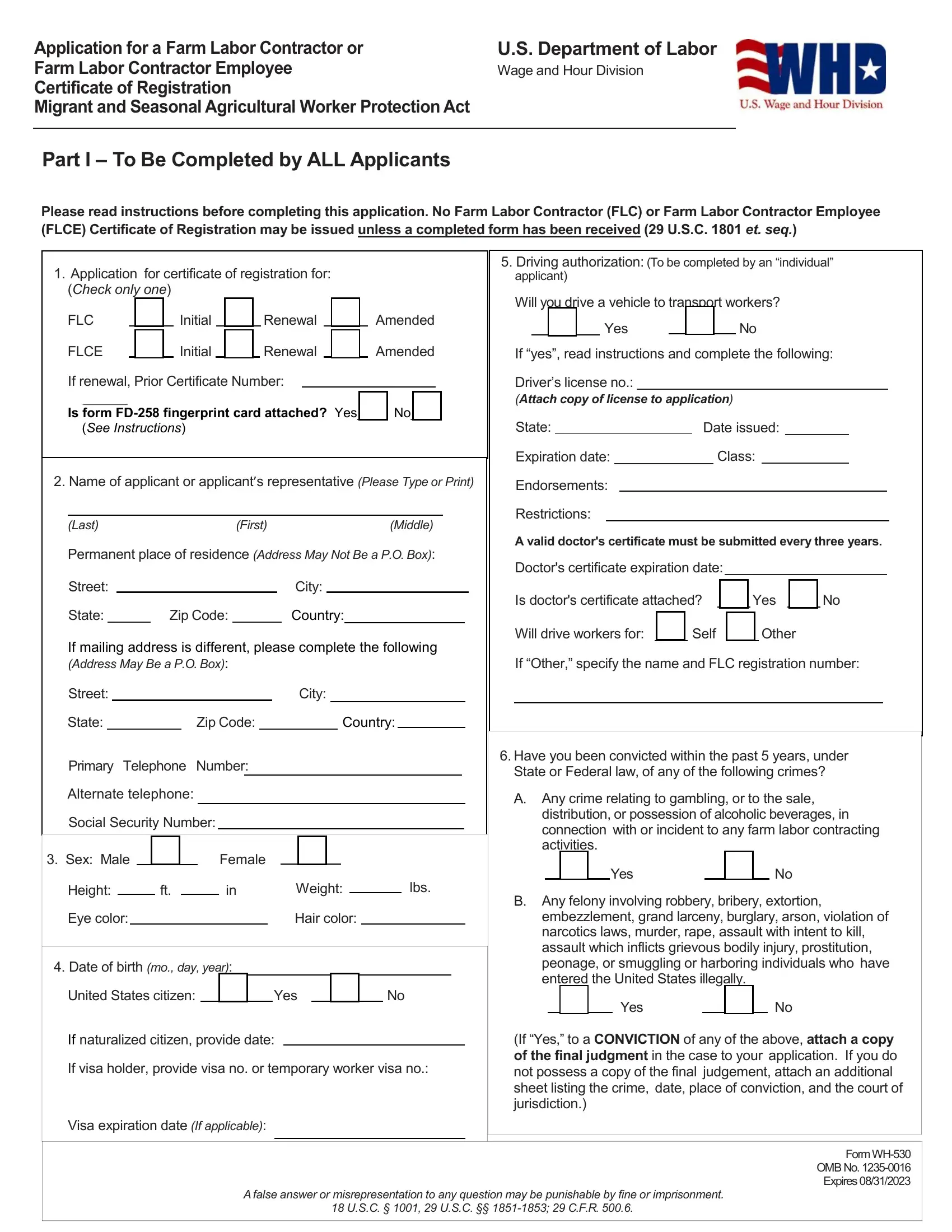
Navigating the intricacies of agricultural employment and legal compliance, the WH-530 form emerges as a crucial document for those seeking to serve as Farm Labor Contractors (FLC) or Farm Labor Contractor Employees (FLCE) under the Migrant and Seasonal Agricultural Worker Protection Act. This comprehensive form, mandated by the U.S. Department of Labor's Wage and Hour Division, requires meticulous completion by all applicants aiming to obtain or renew their certificate of registration. It covers a broad spectrum of information, from personal identification and legal status to details about the services provided, such as hiring, transporting, or housing migrant and seasonal agricultural workers. Additionally, it delves into the applicant's legal background, driving and insurance compliance for transporting workers, and adherence to health and safety standards for any provided housing. This form not only serves as an application but as a declaration of the applicant's intent to comply with all federal and state regulations concerning the safety, compensation, and wellbeing of agricultural workers. With its expiration date carefully noted, the form acts as a testament to the commitment of the Department of Labor to uphold the rights and protections afforded to one of the most vital sectors of the workforce. The careful completion and submission of this form signify the first step in ensuring ethical and legal farm labor contracting practices.
| Question | Answer |
|---|---|
| Form Name | Form Wh 530 |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | labor workers application, labor registration application, form application farm, labor certificate farm |