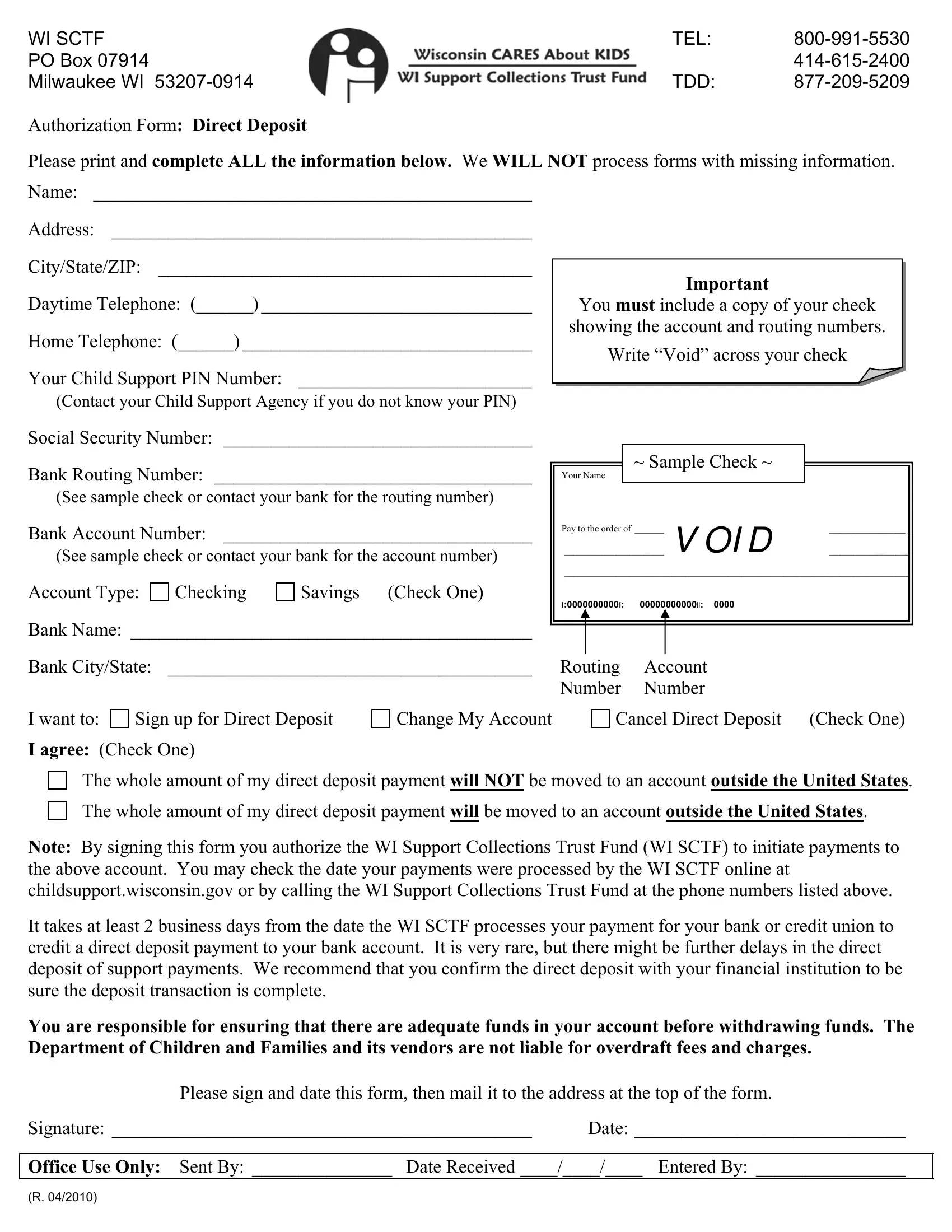
Navigating the complexities of managing child support payments can be streamlined with the Wisconsin Support Collections Trust Fund (WI SCTF) Direct Deposit Authorization Form. This crucial document serves to expedite the process of child support payments, ensuring that funds reach their intended recipients swiftly and securely through direct deposit. To initiate this service, the form mandates the provision of comprehensive personal and banking details, including a voided check to verify account and routing numbers. Moreover, it grants the WI SCTF permission to deposit child support payments directly into the specified bank account, whether it be checking or savings. Applicants have the option to sign up for new direct deposit services, change existing account information, or cancel the service altogether. It's essential to acknowledge that for the form to be processed effectively, all sections must be thoroughly completed; incomplete submissions will not be accepted. Additionally, the form's stipulation that direct deposit payments cannot be transferred internationally unless explicitly agreed upon underscores its commitment to safeguarding financial transactions within the United States. By signing the form, individuals also agree to bear responsibility for any potential overdraft fees, highlighting the importance of ensuring sufficient funds are available in the account prior to making withdrawals. This protocol underscores the WI SCTF's dedication to facilitating a reliable and efficient child support payment system for all parties involved.
| Question | Answer |
|---|---|
| Form Name | Form Wi Sctf |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wisconsin, po box 07914 milwaukee wi, wi sctf p o box 07914 milwaukee wi, overdraft |
WI SCTF |
TEL: |
|
PO BOX 07914 |
|
|
MILWAUKEE WI |
TDD: |
Authorization Form: Direct Deposit
Please print and complete ALL the information below. We WILL NOT process forms with missing information. Name: _______________________________________________
Address: _____________________________________________
City/State/ZIP: ________________________________________
Daytime Telephone: (______) _____________________________
Home Telephone: (______) _______________________________
Your Child Support PIN Number: _________________________
(Contact your Child Support Agency if you do not know your PIN)
Social Security Number: _________________________________
Bank Routing Number: __________________________________ |
Your Name |
~ Sample Check ~ |
|
(See sample check or contact your bank for the routing number)
Bank Account Number: _________________________________ |
Pay to the order of |
___________________________________________________________ |
|
|
V OI D |
||
(See sample check or contact your bank for the account number) |
__________________________________________________________________________ |
||
__________________________________________________________________________ |
|||
|
|||
Account Type:
Checking
Savings |
(Check One) |
L:0000000000L: 00000000000LL: 0000
Bank Name: ___________________________________________ |
|
|
Bank City/State: _______________________________________ |
Routing |
Account |
|
Number |
Number |
I want to: |
Sign up for Direct Deposit |
I agree: (Check One)
Change My Account
Cancel Direct Deposit (Check One)
The whole amount of my direct deposit payment will NOT be moved to an account outside the United States.
The whole amount of my direct deposit payment will be moved to an account outside the United States.
Note: By signing this form you authorize the WI Support Collections Trust Fund (WI SCTF) to initiate payments to the above account. You may check the date your payments were processed by the WI SCTF online at childsupport.wisconsin.gov or by calling the WI Support Collections Trust Fund at the phone numbers listed above.
It takes at least 2 business days from the date the WI SCTF processes your payment for your bank or credit union to credit a direct deposit payment to your bank account. It is very rare, but there might be further delays in the direct deposit of support payments. We recommend that you confirm the direct deposit with your financial institution to be sure the deposit transaction is complete.
You are responsible for ensuring that there are adequate funds in your account before withdrawing funds. The Department of Children and Families and its vendors are not liable for overdraft fees and charges.
Please sign and date this form, then mail it to the address at the top of the form.
Signature: _____________________________________________ Date: _____________________________
Office Use Only: Sent By: _______________ Date Received ____/____/____ Entered By: ________________
(R. 04/2010)