The WKC 16 form, an essential document for the Department of Workforce Development in Wisconsin, plays a pivotal role in the Worker’s Compensation Division process. It is meticulously designed to capture a comprehensive medical report on an industrial injury, ensuring that vital data concerning the worker's condition, the nature of the injury, and the prognosis for recovery are systematically recorded. Situated in Madison, WI, the department handles an array of cases with the primary goal of facilitating the workers' compensation claims efficiently. The form requires detailed information, including personal details of the injured employee, the injury's specifics, diagnosis, and the extent of any permanent disability that may have resulted from the workplace accident. Furthermore, it delves into the history of prior disabilities, if any, and outlines the prognosis for the worker's return to employment, taking into consideration the limitations imposed by the injury. Notably, the form underscores the significance of a thorough evaluation for finger injuries, instructing medical professionals to use statutory terms and precise measurements to assess the loss of use or motion. This meticulous approach to data collection not only aids in the fair assessment of claims but also underscores the department’s commitment to protecting workers’ rights and wellbeing.
| Question | Answer |
|---|---|
| Form Name | Form Wkc 16 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form wkc 16, wkc 16 wisconsin, wkc 16, wkc 16 blank form |

MEDICAL REPORT ON INDUSTRIAL INJURY
Department of Workforce Development Worker’s Compensation Division
201 E. Washington Ave., Rm. C100 P.O. Box 7901
Madison, WI
Telephone: (608)
Fax: (608)
Provision of your Social Security Number (SSN) is voluntary. Failure to provide it may result in an information processing delay. Personal information you provide may be used for secondary purposes [Privacy Law, s. 15.04 (1)(m), Wisconsin Statutes].
|
WC Claim Number |
Employee Name |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
PATIENT |
Employee Social Security Number |
Employee Address |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Injury |
|
|
|
|
|
|
|
|
|
|
Date |
|
Employer Name |
|
|
|
Insurance Company |
|
|||
|
|
|
|
|
|
|
|
|
|
|
HISTORY |
History as described by patient |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DIAGNOSIS |
|
|
|
|
|
|
|
|
|
|
(Please be as |
|
|
|
|
|
|
|
|
|
|
detailed as |
|
|
|
|
|
|
|
|
|
|
possible) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
PERMANENT |
What amputation present? |
Comparative |
|
Stump: |
|
|||||
|
|
|
Ye s |
No |
|
|
hardy or |
tender |
||
DISABILITY |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
(Describe permanent |
Has permanent disability resulted? |
Date of Last Exam |
|
Has healing period ended? |
Patient discharged? |
|||||
elements of disability, |
Yes |
No |
|
|
|
Ye s |
No |
|
Ye s |
No |
such as limitation of |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
motion, pain, weakness, |
Description of permanent disability (Record finger motion losses on reverse.) |
|
|
|
||||||
etc., and describe effect |
|
|
|
|
|
|
|
|
|
|
on working ability.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Was surgery performed as a result of accident? |
Ye s |
|
No |
If Yes, state type of surgery: |
|
||||
|
|
|
|
|
||||||
|
If healing has not ended, what is minimum permanent disability expected? |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
PRIOR |
What previous disability? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISABILITY |
|
|
|
|
|
|
|
|
|
|
PROGNOSIS |
Prognosis: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Date injured was or will be able to return to a limited type of work: |
|
|
|
|
|||||
|
State any limitations: |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Date injured was or will be able to return to |
|
||||||||
|
|
|
|
|
|
|
|
|
||
|
What further treatment should be given? |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Additional comments, if any:
Date |
City |
|
|
Physician or Chiropractor Signature (in own writing) |
|
|
|
||
|
Phone Number |
Typed or Printed Name |
||
|
( |
) |
- |
|
|
|
|
|
|
Employee Name
Employee Social Security Number
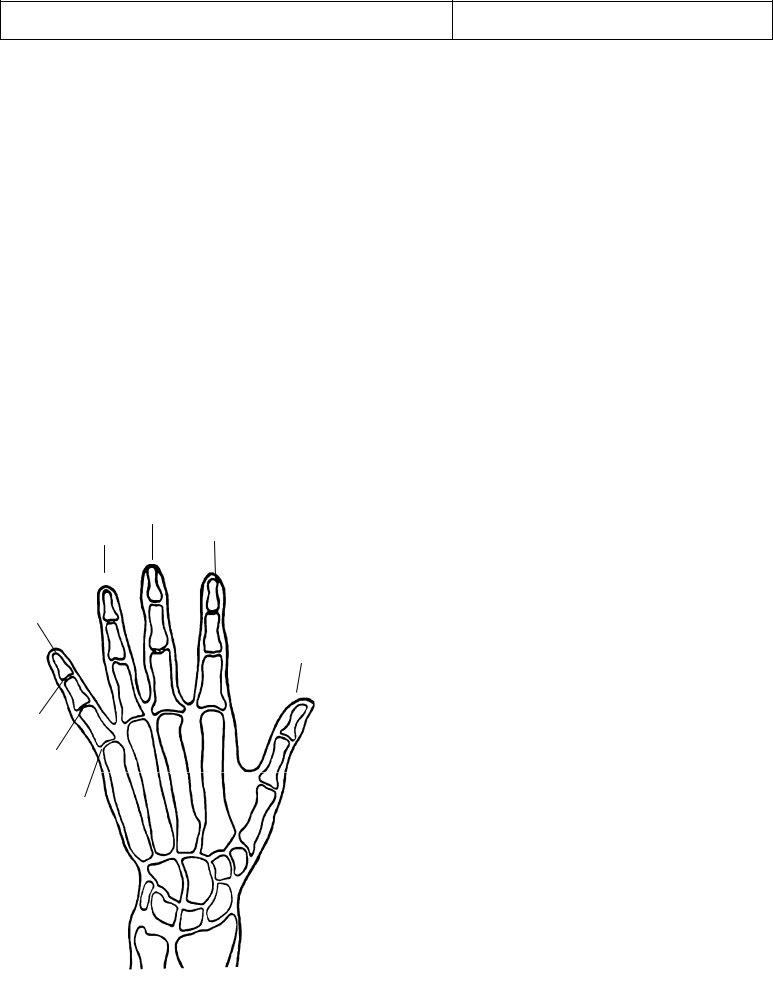
Instructions for finger injuries
Please use statutory terms in referring to fingers, such as thumbs, index, middle, ring, and little fingers, and distal, middle, and proximal joints. Where there is limitation of motion, list separately the normal range of motion in degrees, the “degrees” loss of flexion, and the “degrees” loss of extension for each joint of each finger. The Worker’s Compensation Division will evaluate the loss of use due to loss of motion of the fingers.
Where there are other elements of disability of the fingers, such as deformity, weakness, pain, or lack of endurance, give your opinion on the percentage loss of use as compared to amputation for such elements of disability and specify the joint at which such loss is estimated.
|
|
Angle |
Normal |
Degrees |
Degrees |
Estimate % loss of use for additional factors at joint |
|
Digit |
Joint |
Range of |
Loss |
Loss |
|||
Ext./Flex |
involved and reason for additional allowance |
||||||
|
|
Motion |
Extension |
Flexion |
|||
|
|
|
|
||||
Thumb |
Dist |
|
|
|
|
|
|
|
Prox |
|
|
|
|
|
|
Index |
Dist |
|
|
|
|
|
|
|
Mid |
|
|
|
|
|
|
|
Prox |
|
|
|
|
|
|
Mid |
Dist |
|
|
|
|
|
|
|
Mid |
|
|
|
|
|
|
|
Prox |
|
|
|
|
|
|
Ring |
Dist |
|
|
|
|
|
|
|
Mid |
|
|
|
|
|
|
|
Prox |
|
|
|
|
|
|
Little |
Dist |
|
|
|
|
|
|
|
Mid |
|
|
|
|
|
|
|
Prox |
|
|
|
|
|
CIRCLE HAND INVOLVED: Right Left
Middle Finger
DOMINANT HAND: Right |
Left |
Ring Finger
Little Finger
Distal
Joint
Middle
Joint
Proximal
Joint
Index Finger
Thumb
See DWD 80.32 & 80.33 for guides to evaluation for amputations, restrictions of motion, ankylosis, sensory loss, and surgical results for disability to the hip, knee, ankle, toes, shoulder, elbow, wrist, fingers and back.
If fingertip amputation is present, submit comparative
If amputation is below the distal joint, submit comparative