
When you desire to fill out care form, you won't have to download any sort of applications - simply try using our PDF editor. Our team is ceaselessly endeavoring to improve the tool and ensure it is much faster for clients with its extensive functions. Discover an constantly progressive experience now - explore and discover new possibilities as you go! All it requires is a few easy steps:
Step 1: Firstly, access the editor by pressing the "Get Form Button" at the top of this site.
Step 2: With this handy PDF file editor, it's possible to accomplish more than just fill in forms. Express yourself and make your docs appear professional with customized textual content incorporated, or adjust the original content to perfection - all that comes along with the capability to add stunning pictures and sign the PDF off.
When it comes to blanks of this precise PDF, this is what you should consider:
1. The care form involves particular details to be typed in. Make certain the subsequent blanks are filled out:
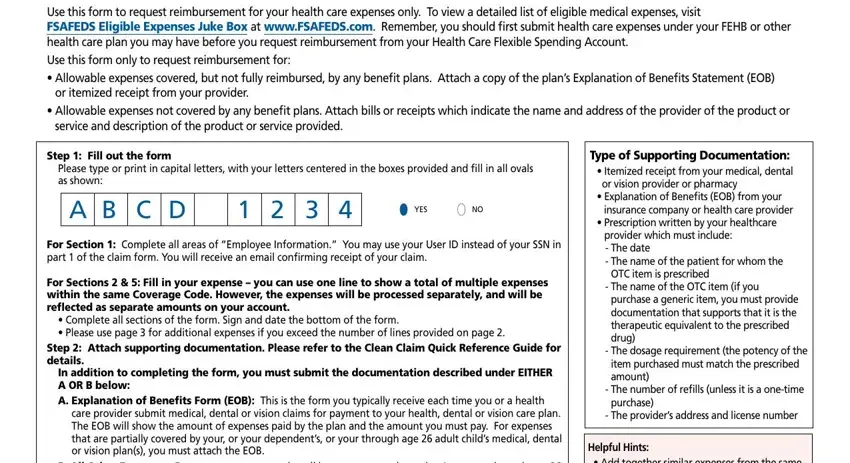
2. Soon after the previous part is filled out, go on to enter the suitable information in these: Usecodeforanyeligibleitemthatisnt, Questions Need a list of eligible, and Page HEALTH CARE CLAIM FORM.

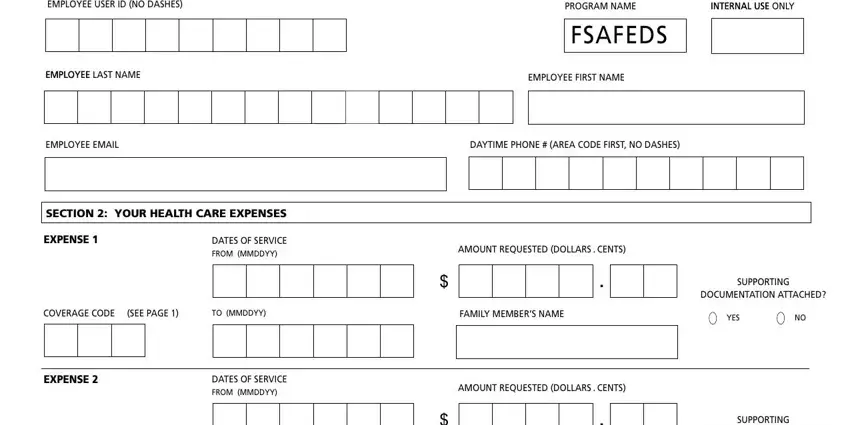
3. The following segment should be fairly straightforward, FSAFEDS, SECTION YOUR HEALTH CARE EXPENSES, EXPENSE, DATES OF SERVICE FROM MMDDYY, COVERAGE CODE, SEE PAGE, EXPENSE, DATES OF SERVICE FROM MMDDYY, SUPPORTING, YES, and SUPPORTING - all of these form fields must be filled out here.
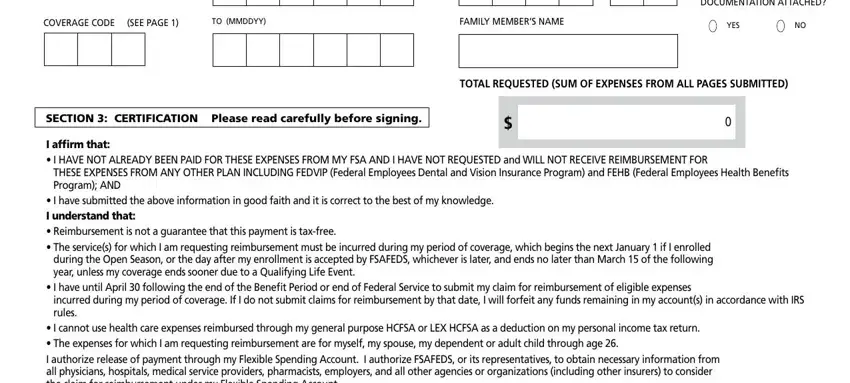
4. Your next section requires your details in the following places: COVERAGE CODE, SEE PAGE, YES, SECTION CERTIFICATION Please read, TOTAL REQUESTED SUM OF EXPENSES, and I affirm that I. Make sure that you give all of the needed details to move onward.
5. While you near the completion of this form, there are a few more things to undertake. In particular, I affirm that I, Employee Signature Your signature, Date MMDDYY, Page HEALTH CARE CLAIM FORM, and WKBVDY must be filled in.

Always be extremely attentive when completing Employee Signature Your signature and Page HEALTH CARE CLAIM FORM, because this is the part in which a lot of people make some mistakes.
Step 3: Just after looking through your form fields you've filled in, click "Done" and you're done and dusted! Find your care form as soon as you register online for a 7-day free trial. Immediately view the pdf inside your FormsPal account, along with any edits and changes being conveniently preserved! Here at FormsPal.com, we endeavor to make certain that your information is maintained private.