
Using PDF files online is always simple with our PDF editor. Anyone can fill in Marfan here without trouble. Our tool is constantly developing to provide the very best user experience achievable, and that is thanks to our commitment to continual improvement and listening closely to customer opinions. Starting is effortless! What you need to do is follow these basic steps down below:
Step 1: Hit the "Get Form" button above. It will open our tool so you can begin filling in your form.
Step 2: When you start the editor, you will get the document made ready to be filled out. Aside from filling out various blanks, you might also perform other things with the PDF, namely putting on your own textual content, modifying the original text, adding graphics, affixing your signature to the document, and much more.
Be attentive when filling out this pdf. Ensure all mandatory blanks are filled out properly.
1. While filling out the Marfan, make certain to complete all essential blank fields within the relevant area. This will help to expedite the process, making it possible for your details to be handled fast and properly.
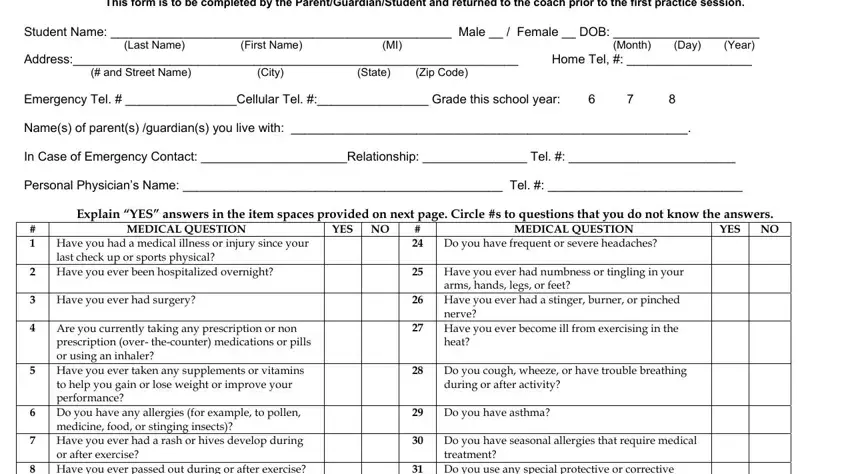
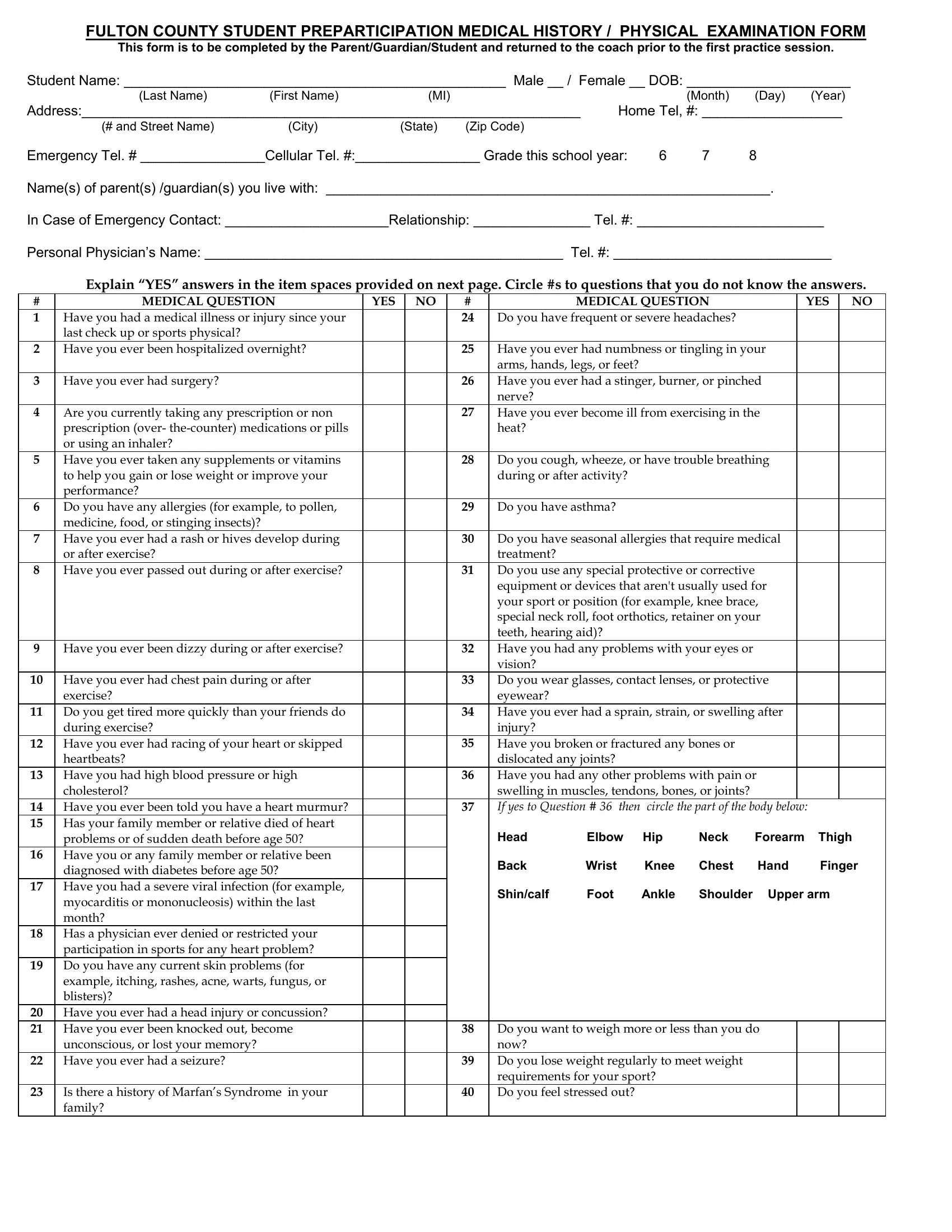
2. Once your current task is complete, take the next step – fill out all of these fields - Have you ever passed out during, Have you ever been dizzy during, Have you ever had chest pain, exercise, Do you get tired more quickly, during exercise, Have you ever had racing of your, heartbeats, Have you had high blood pressure, cholesterol, Have you ever been told you have, problems or of sudden death before, Have you or any family member or, diagnosed with diabetes before age, and Have you had a severe viral with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
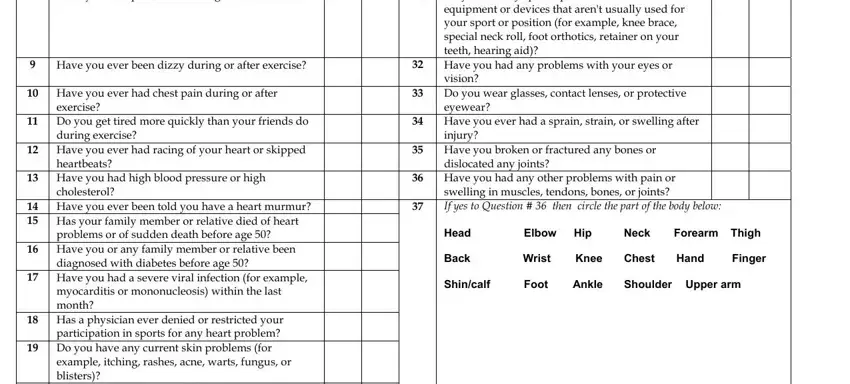
3. This 3rd step should be quite straightforward, Have you ever had a head injury, unconscious or lost your memory, Have you ever had a seizure, Is there a history of Marfans, and Do you want to weigh more or less - each one of these blanks needs to be filled out here.
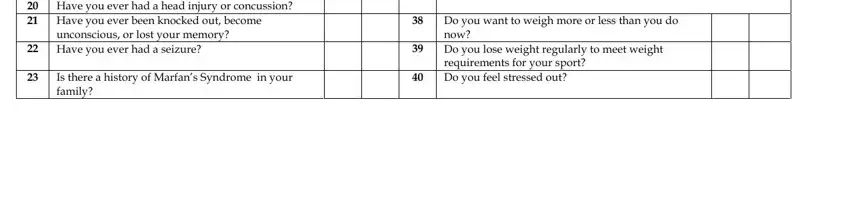
As to Do you want to weigh more or less and Have you ever had a seizure, be sure you get them right in this section. Those two are the key ones in this page.
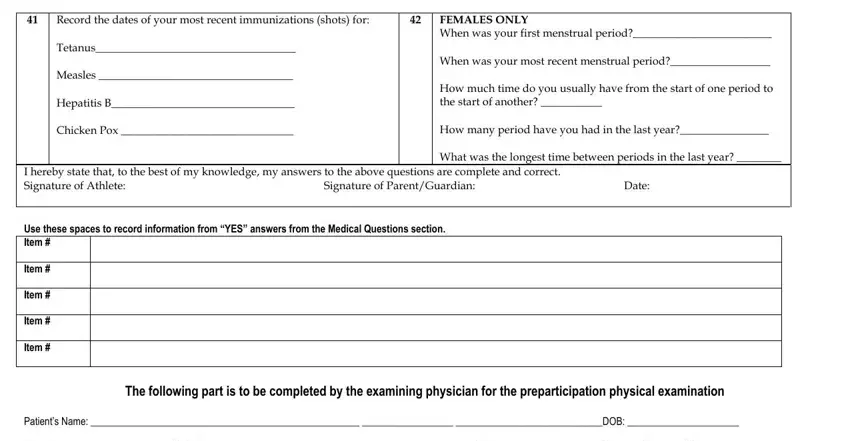
4. This next section requires some additional information. Ensure you complete all the necessary fields - Record the dates of your most, FEMALES ONLY When was your first, Signature of ParentGuardian, I hereby state that to the best of, Date, The following part is to be, and Patients Name DOB Height - to proceed further in your process!
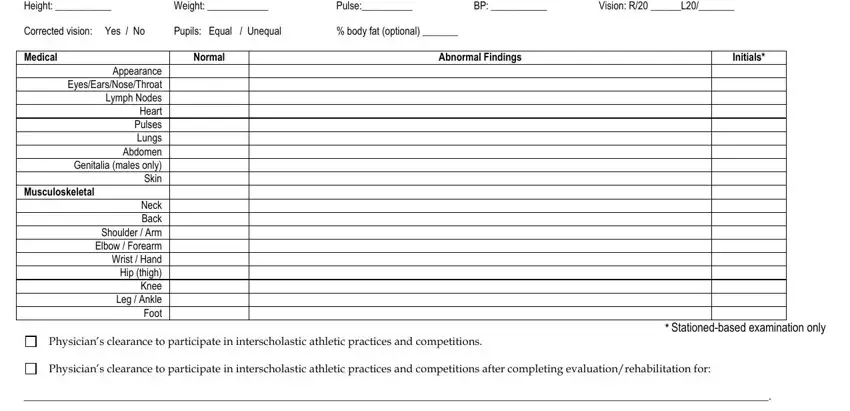
5. This document should be concluded by dealing with this section. Here you'll see an extensive set of form fields that require accurate details for your document usage to be faultless: Patients Name DOB Height, Vision R L, body fat optional, Pupils Equal Unequal, Weight, Abnormal Findings, Pulse, Normal, Initials, Appearance EyesEarsNoseThroat, Musculoskeletal, Neck Back Shoulder Arm Elbow, Stationedbased examination only, Physicians clearance to, and Physicians clearance to.
Step 3: You should make sure your information is accurate and then click on "Done" to complete the project. Acquire the Marfan after you join for a free trial. Immediately use the pdf form in your FormsPal account, with any modifications and changes all kept! When you use FormsPal, you can complete documents without stressing about information incidents or records being shared. Our protected platform makes sure that your private data is stored safe.