
functional capacity evaluation form can be filled out without any problem. Just try FormsPal PDF editing tool to get it done promptly. FormsPal is dedicated to making sure you have the best possible experience with our editor by continuously releasing new features and upgrades. With all of these updates, working with our tool becomes easier than ever! To get the process started, take these easy steps:
Step 1: Simply hit the "Get Form Button" in the top section of this page to open our pdf form editor. There you'll find all that is needed to work with your file.
Step 2: With this online PDF tool, you can accomplish more than simply fill out blank fields. Edit away and make your forms appear sublime with customized textual content put in, or adjust the file's original content to excellence - all that accompanied by the capability to insert stunning pictures and sign it off.
Completing this PDF usually requires attentiveness. Make certain all mandatory fields are done properly.
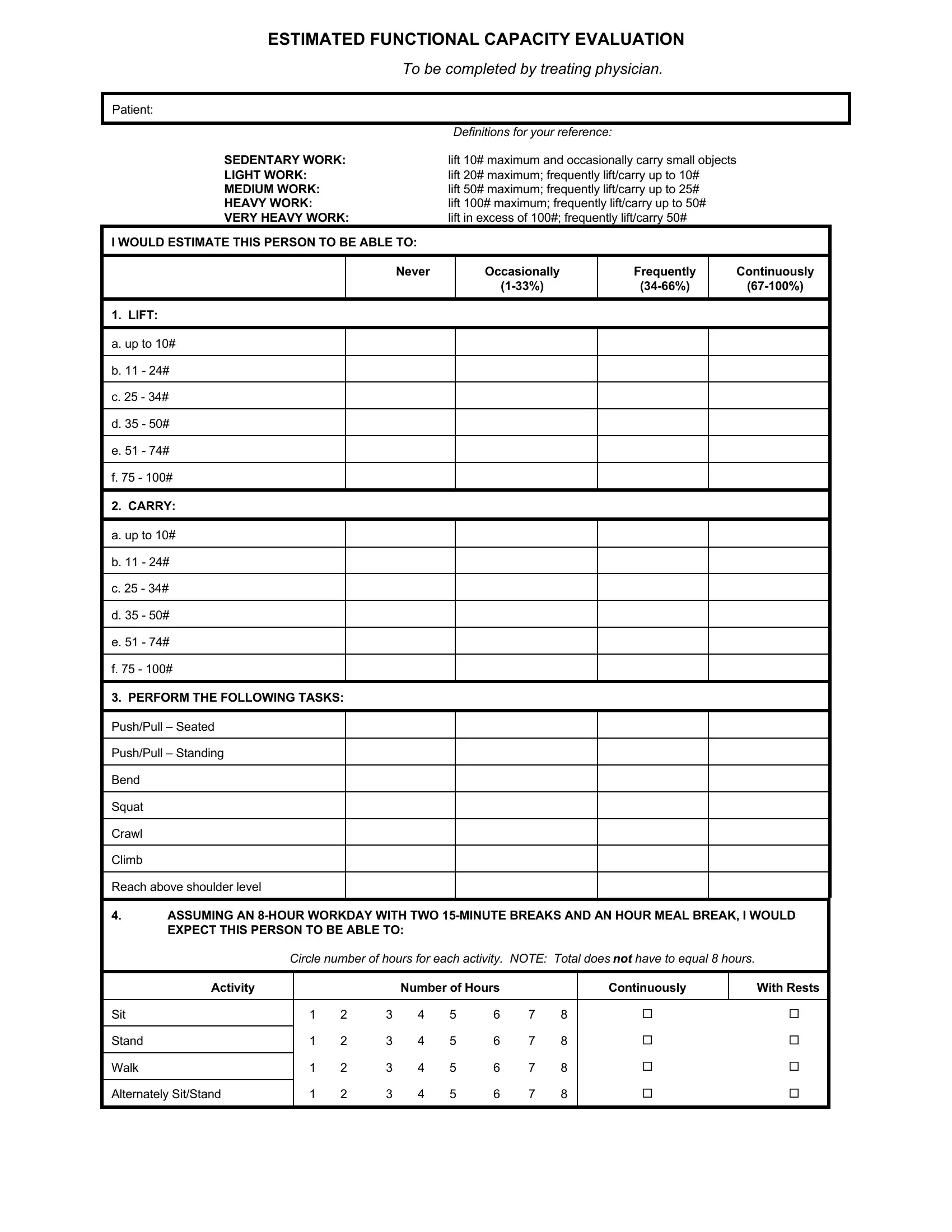
1. Complete your functional capacity evaluation form with a group of major blanks. Note all of the required information and make certain nothing is overlooked!
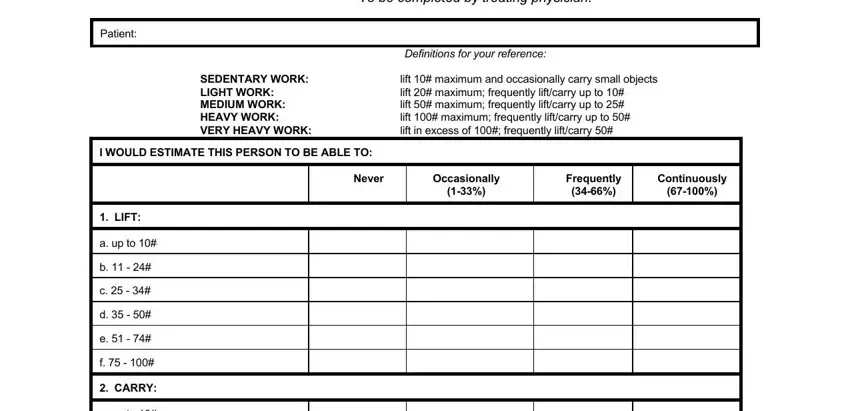
2. After this section is done, you're ready put in the needed details in a up to, PERFORM THE FOLLOWING TASKS, PushPull Seated, PushPull Standing, Bend, Squat, Crawl, Climb, Reach above shoulder level, ASSUMING AN HOUR WORKDAY WITH TWO, Circle number of hours for each, Sit, Stand, Walk, and Activity so you're able to go further.
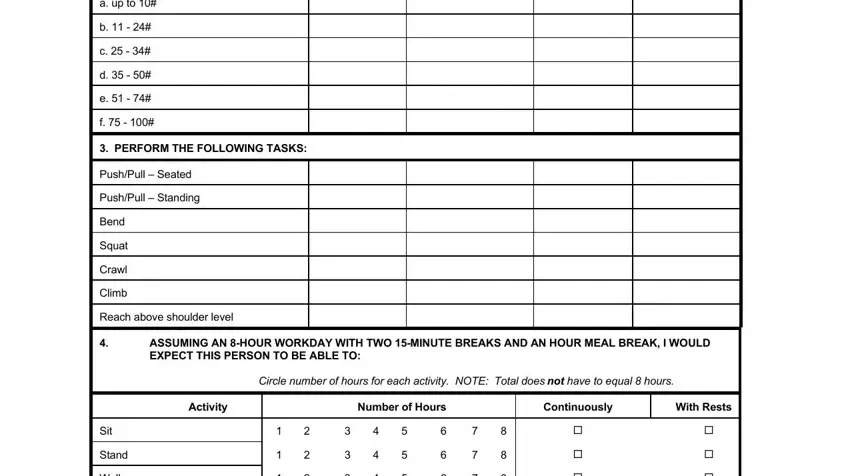
3. In this particular stage, look at Walk, and Alternately SitStand. These are required to be filled out with highest accuracy.

4. To go ahead, the next stage will require filling out a few empty form fields. These include Right, Left, Simple Grasping, Yes, Yes, Firm Grasping, Yes, Yes, Fine Manipulating, Yes, Yes, Estimated Grip Strength Right, CAN PERSON USE FEET FOR REPETITIVE, Right Alone, and Yes, which are fundamental to moving forward with this particular form.
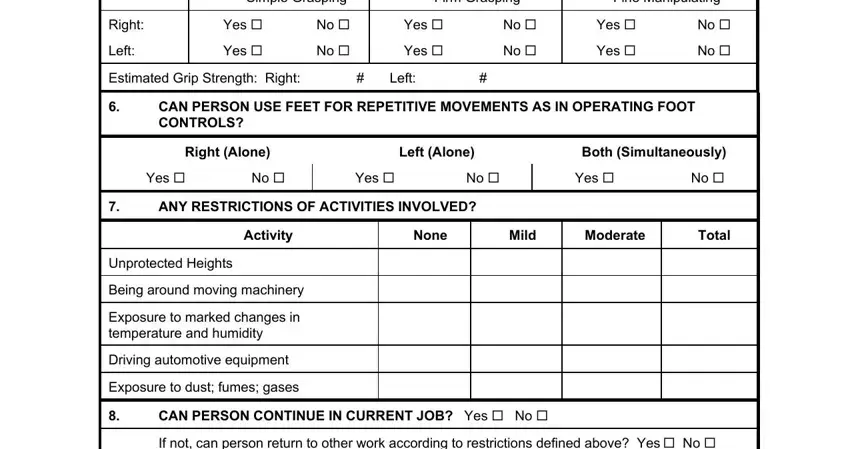
As to Yes and Yes, make sure that you don't make any errors here. These two are surely the most important ones in the PDF.
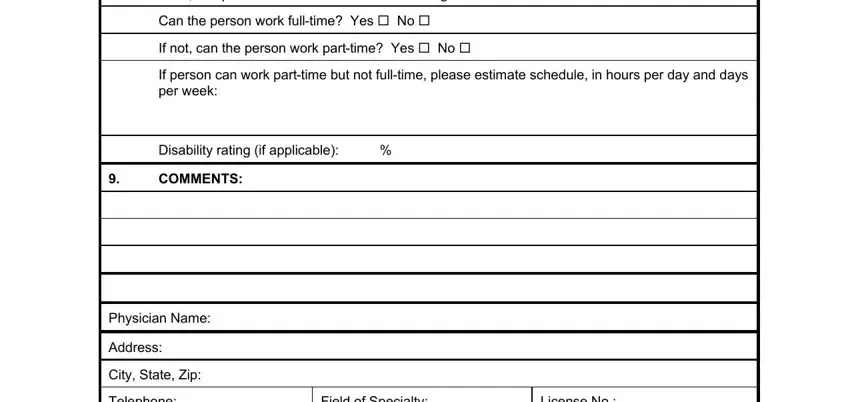
5. This document has to be finalized by going through this area. Further there can be found a comprehensive set of blank fields that require correct details in order for your form submission to be complete: If not can person return to other, Can the person work fulltime Yes, If not can the person work, If person can work parttime but, Disability rating if applicable, COMMENTS, Physician Name, Address, City State Zip, Telephone, Field of Specialty, and License No.
Step 3: Ensure the details are correct and then just click "Done" to progress further. Obtain the functional capacity evaluation form when you sign up for a free trial. Easily view the pdf inside your personal cabinet, along with any edits and adjustments being conveniently synced! At FormsPal.com, we strive to make sure all your details are stored private.