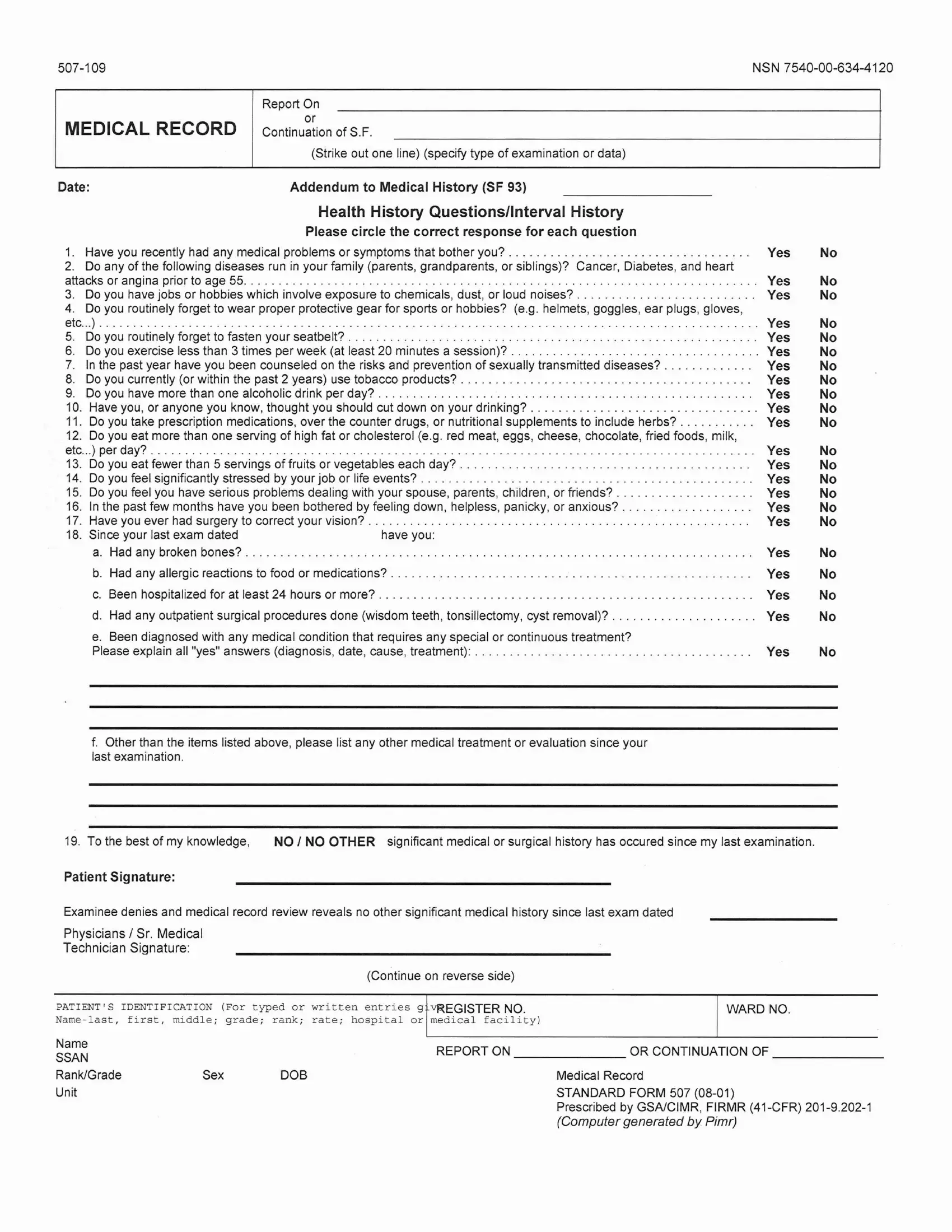
The Standard 507 form serves as a critical tool in the medical field, particularly for comprehensive recording and continuation of medical histories, examination data, and health assessments. It meticulously gathers personal health history, family medical history, lifestyle habits, and potential risk factors that could impact an individual's health status. Specifically designed to augment the Medical History Form (SF 93), the Standard 507 form delves into detailed questions about recent medical issues, genetic diseases prevalent in the family, and behaviors that could predispose individuals to health risks, such as exposure to hazardous materials, neglect in the use of protective gear, unhealthy dietary habits, substance use, and inadequate physical activities. Moreover, it addresses mental health concerns, stressing the significance of acknowledging and addressing symptoms related to stress, depression, anxiety, and relational problems. The process for completing this form is meticulous, requiring truthful and comprehensive responses to each enumerated query, with clear instructions provided for explaining any affirmative answer in detail. This systematic approach ensures that healthcare providers get a well-rounded view of the examinee’s health, guiding them in offering personalized care and preventive measures tailored to the individual's needs and health risks. The form underscores the importance of transparency and accuracy in reporting medical information, thereby facilitating better health outcomes for individuals.
| Question | Answer |
|---|---|
| Form Name | Standard Form 507 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form om 501, google army form sf 507, sf 507 blank, online version of word |
