
military form 507 can be filled out online effortlessly. Just open FormsPal PDF editing tool to get the job done quickly. FormsPal is committed to giving you the best possible experience with our tool by regularly presenting new functions and improvements. Our editor is now much more helpful as the result of the newest updates! Now, working with PDF documents is easier and faster than before. Getting underway is easy! All you should do is take the following easy steps below:
Step 1: Access the form in our tool by pressing the "Get Form Button" at the top of this page.
Step 2: Once you launch the PDF editor, you will get the form ready to be filled in. Other than filling in various blank fields, it's also possible to do some other actions with the form, namely writing your own textual content, modifying the initial text, adding graphics, affixing your signature to the PDF, and more.
It's straightforward to complete the pdf following this practical tutorial! Here's what you want to do:
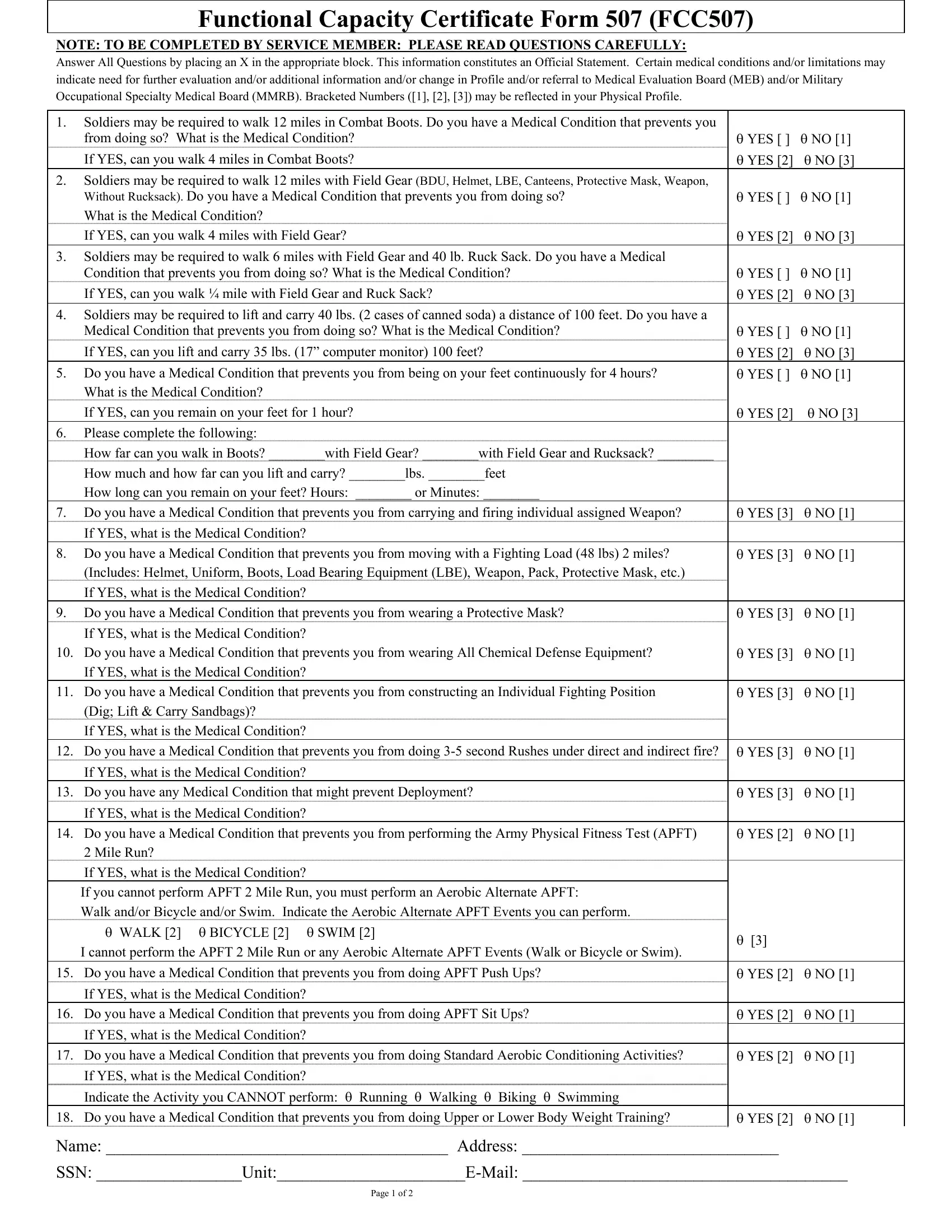
1. The military form 507 will require certain information to be inserted. Ensure the subsequent blank fields are filled out:
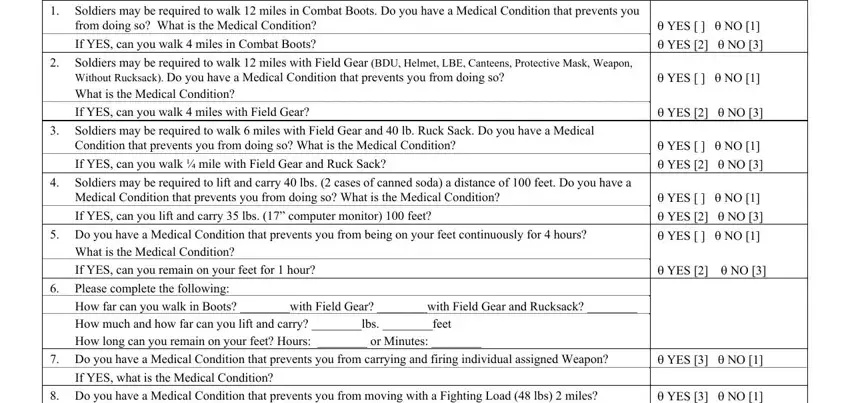
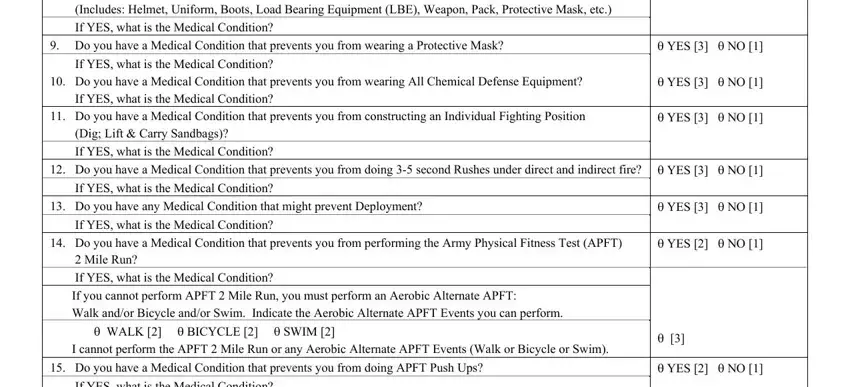
2. Right after filling out the previous step, head on to the next part and complete all required details in all these blanks - Do you have a Medical Condition, Includes Helmet Uniform Boots Load, If YES what is the Medical, Do you have a Medical Condition, If YES what is the Medical, Do you have a Medical Condition, If YES what is the Medical, Do you have a Medical Condition, Dig Lift Carry Sandbags, YES NO YES NO , YES NO YES NO , YES NO , If YES what is the Medical, Do you have any Medical Condition, and If YES what is the Medical.
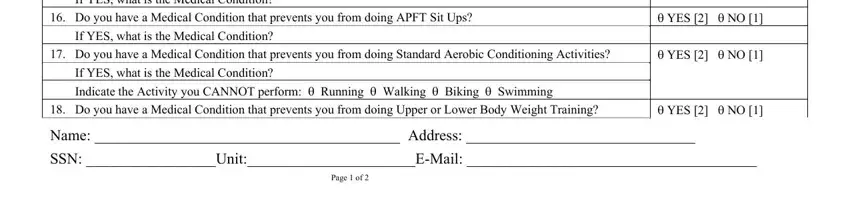
3. The following portion is focused on If YES what is the Medical, Do you have a Medical Condition, If YES what is the Medical, Do you have a Medical Condition, If YES what is the Medical, YES NO YES NO YES NO , YES NO , Name Address , SSN UnitEMail , and Page of - fill out these empty form fields.
A lot of people often make mistakes when completing YES NO in this section. You should reread everything you enter right here.
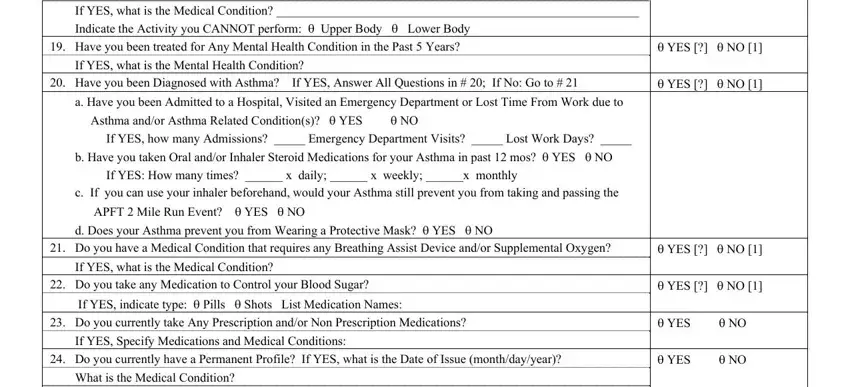
4. Filling in If YES what is the Medical, If YES what is the Mental Health, Have you been Diagnosed with, a Have you been Admitted to a, c If you can use your inhaler, If YES what is the Medical, Do you take any Medication to, YES NO YES NO , YES NO YES NO YES NO, and If YES Specify Medications and is paramount in the fourth step - ensure that you spend some time and be attentive with every single blank area!
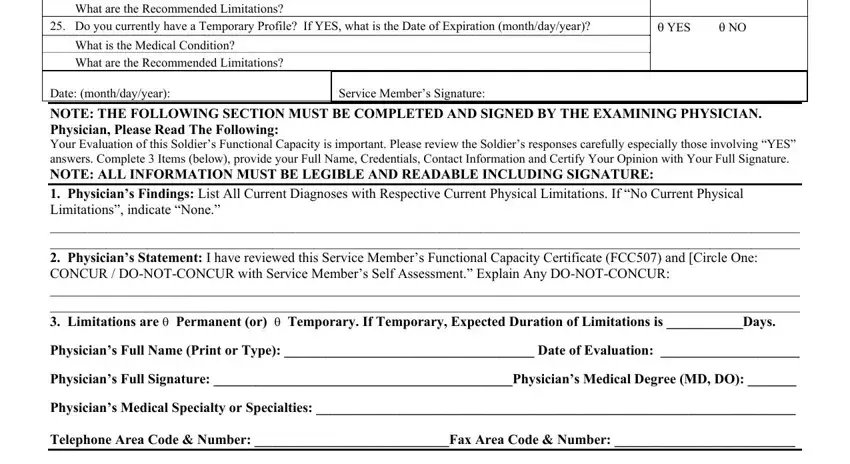
5. To finish your form, the final section includes some additional fields. Filling in What are the Recommended, Do you currently have a Temporary, What is the Medical Condition, What are the Recommended, Service Members Signature, YES NO, NOTE THE FOLLOWING SECTION MUST BE, and Physicians Findings List All will finalize the process and you'll be done in the blink of an eye!
Step 3: Right after you have looked once again at the information you given, just click "Done" to conclude your document creation. Join us right now and immediately use military form 507, available for download. Every change you make is conveniently kept , which enables you to modify the file at a later stage if needed. We do not sell or share the details that you type in while filling out forms at our website.