
Handling PDF forms online is actually very simple with this PDF tool. You can fill out illinois funeral reimbursement here in a matter of minutes. To maintain our editor on the forefront of efficiency, we work to adopt user-oriented capabilities and enhancements regularly. We're always looking for feedback - play a vital role in remolding the way you work with PDF documents. Here's what you'll want to do to start:
Step 1: Press the orange "Get Form" button above. It'll open up our pdf tool so you could begin filling out your form.
Step 2: After you access the online editor, you will get the document made ready to be filled in. Besides filling out various blanks, it's also possible to do various other actions with the form, that is adding any textual content, editing the initial text, adding graphics, affixing your signature to the document, and much more.
This document will require specific information; to guarantee correctness, you need to bear in mind the following recommendations:
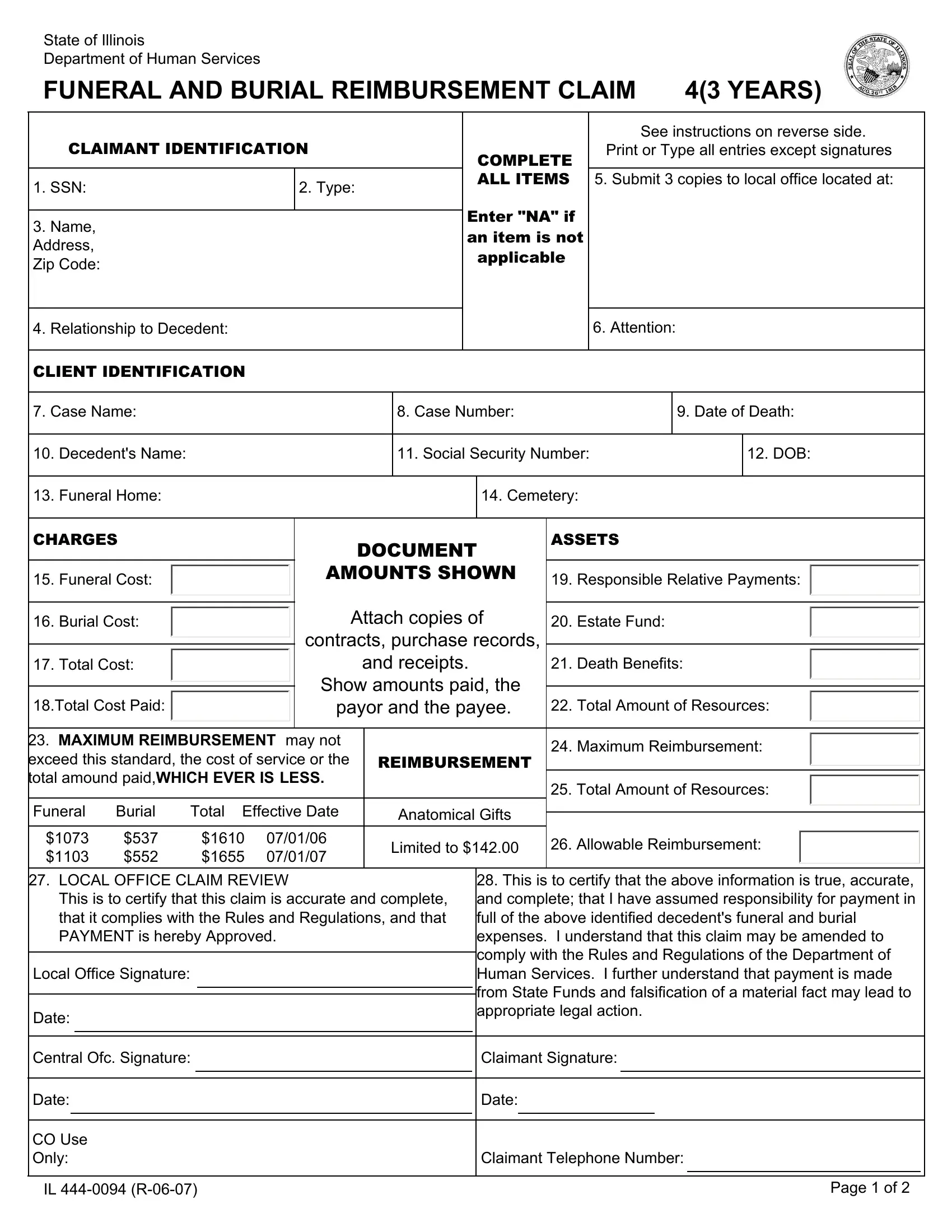
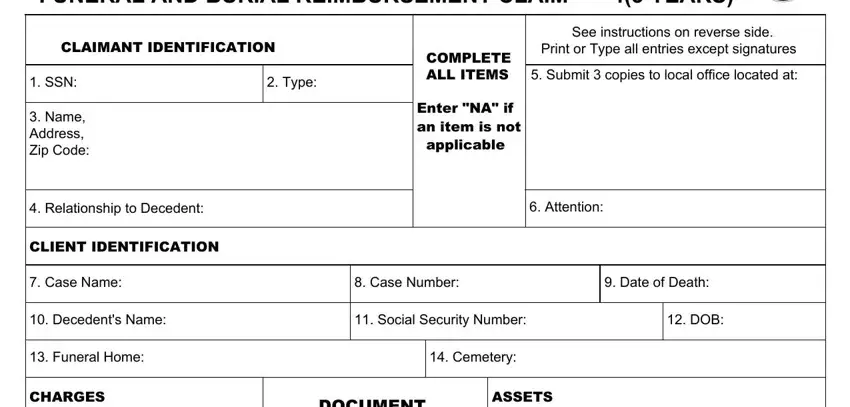
1. The illinois funeral reimbursement needs particular details to be entered. Be sure that the subsequent blanks are completed:
2. After the previous array of fields is finished, you need to add the needed details in Funeral Cost, Burial Cost, Total Cost, Total Cost Paid, DOCUMENT AMOUNTS SHOWN, Attach copies of contracts, MAXIMUM REIMBURSEMENT may not, REIMBURSEMENT, Funeral Burial Total Effective Date, Anatomical Gifts, Responsible Relative Payments, Estate Fund, Death Benefits, Total Amount of Resources, and Maximum Reimbursement in order to proceed to the next stage.
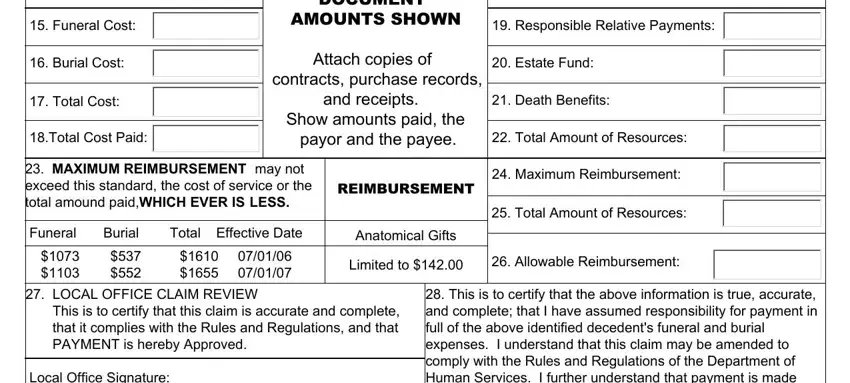
It is easy to get it wrong when filling out your Death Benefits, so make sure you look again prior to deciding to send it in.
3. The following part is related to Local Office Signature, Date, This is to certify that the above, Central Ofc Signature, Claimant Signature, Date, CO Use Only, IL R, Date, Claimant Telephone Number, and Page of - complete each one of these empty form fields.
Step 3: Once you have reviewed the information you given, simply click "Done" to conclude your document generation. Sign up with FormsPal today and immediately access illinois funeral reimbursement, available for download. All changes made by you are saved , letting you change the form at a later time anytime. If you use FormsPal, you can fill out documents without having to get worried about personal data breaches or entries being distributed. Our secure system makes sure that your personal data is kept safely.