We chose the top-rated website developers to create our PDF editor. This app will let you fill in the application for ged file simply and won't require a great deal of your energy. This convenient guideline can assist you to get going.
Step 1: The first step should be to choose the orange "Get Form Now" button.
Step 2: As you get into our application for ged editing page, you'll see each of the functions you may take about your form within the top menu.
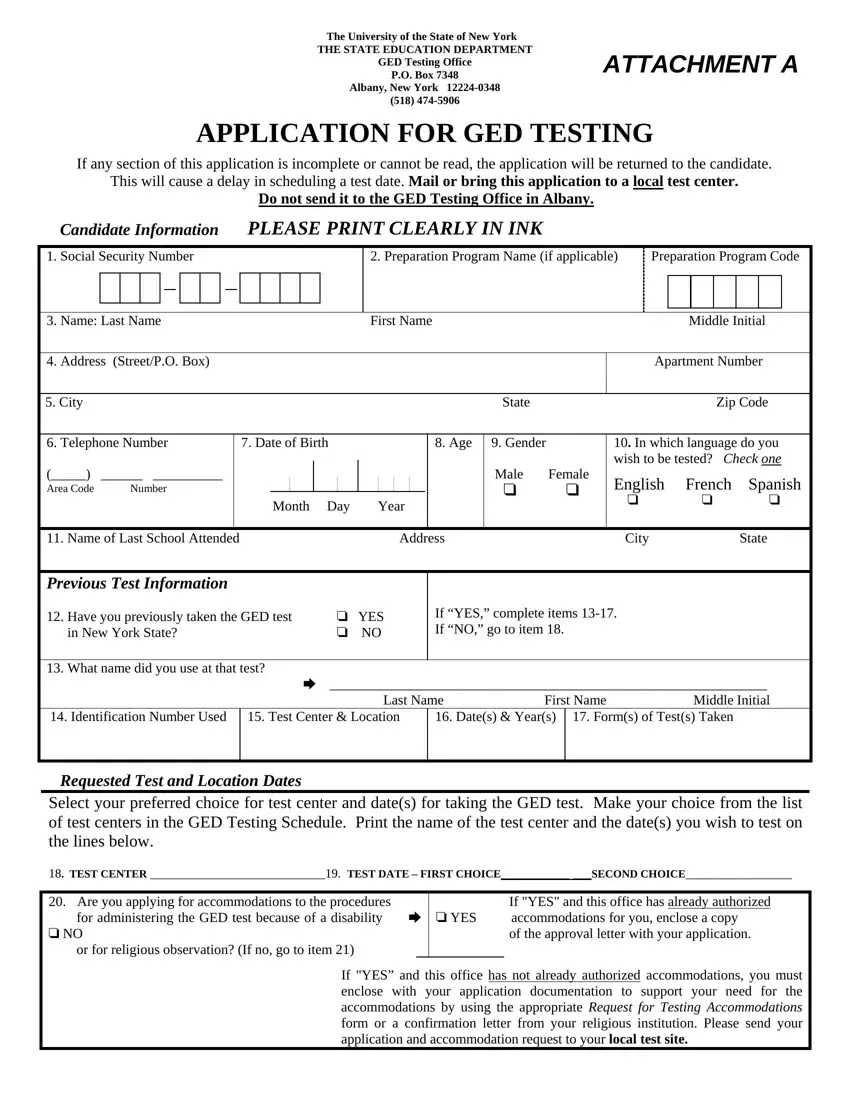
Provide the content demanded by the application to prepare the file.
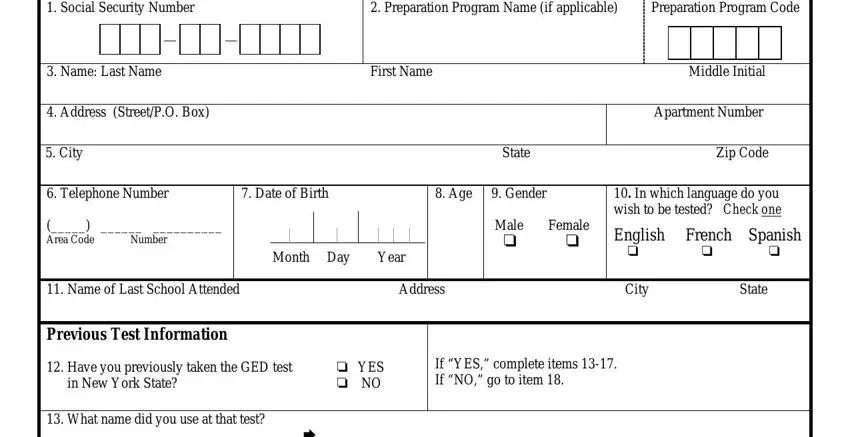
Provide the demanded details in the What name did you use at that, Dates Years Forms of Tests Taken, Test Center Location, Requested Test and Location Dates, Select your preferred choice for, TEST CENTER TEST DATE FIRST, Are you applying for, If YES and this office has already, and If YES and this office has not segment.
Describe the most vital information about the Eligibility Information Are you, Eligibility for persons under the, If NO go to item You must obtain, Please use a check mark cid to, cid B One year has passed since, time high school program of, cid B You were a member of a high, Program or, cid BCYou have been accepted into, university or accredited post, cid B You are a member of the Job, and probation officer field.
Please make sure to write down the rights and obligations of the sides in the probation officer, cid B You are at least and have, You must also have reached maximum, Permission to Release GED Test, cid YES cid NO preparation, Do you give permission to have, CANDIDATE SIGNATURE DATE, CertificationAffidavit, I understand that my eligibility, on any enclosed documentation If, and CANDIDATE SIGNATURE DATE paragraph.
Check the areas CANDIDATE SIGNATURE DATE, Permission of ParentGuardian if, By signing below I am verifying, sondaughter circle one named to, and PARENT SIGNATURE DATE and then fill them out.
Step 3: Press the "Done" button. Now it's easy to export your PDF form to your electronic device. Additionally, you can send it via electronic mail.
Step 4: Create copies of your file - it may help you refrain from forthcoming concerns. And don't worry - we don't share or check the information you have.
