Handful of tasks are simpler than managing documentation through our PDF editor. There isn't much you should do to edit the how to geico form application file - only adopt these measures in the next order:
Step 1: Choose the orange "Get Form Now" button on the following page.
Step 2: At this point, you can alter the how to geico form application. Our multifunctional toolbar helps you include, remove, adjust, highlight, as well as undertake other sorts of commands to the words and phrases and areas inside the form.
All of the following segments are going to make up the PDF file:
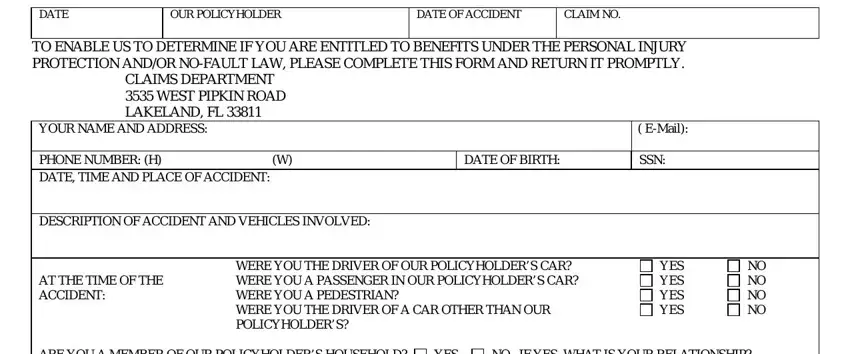
Please type in the appropriate details in the ARE YOU A MEMBER OF OUR, YES, YES, NO IF YES WHAT IS YOUR, SIGN HERE AND RETURN THIS FORM TO, Signature, DATE, DESCRIBE YOUR INJURY, DID A DOCTOR TREAT YOU, YES, NO DOCTORS NAME AND ADDRESS, IF YOU WERE TREATED IN A HOSPITAL, INPATIENT, OUTPATIENT, and HOSPITALS NAME AND ADDRESS area.
Write the necessary particulars in DID YOU LOSE WAGES AS A RESULT OF, YES, IF YES AMOUNT LOST TO DATE, WHAT IS YOUR AVERAGE WEEKLY WAGE, DATE DISABILITY FROM WORK BEGAN, DATE YOU RETURNED TO WORK, YES YES YES, NO NO NO, IF YES AMOUNT CHOOSE ONE PER WEEK, SEE REVERSE SIDE, and C FL area.
The NAME AND ADDRESS OF YOUR PRESENT, AS A RESULT OF YOUR INJURY HAVE, YES, NO IF YES EXPLAIN, SIGNATURE DATE, IMPORTANT TO BE ELIGIBLE FOR, COMPLETE AND SIGN THIS, and FOR YOUR PROTECTION FLORIDA LAW field could be used to indicate the rights and responsibilities of each side.
Step 3: Select the Done button to save the document. At this point it is at your disposal for transfer to your device.
Step 4: You can generate duplicates of the file toprevent different potential concerns. Don't be concerned, we do not display or track your data.
