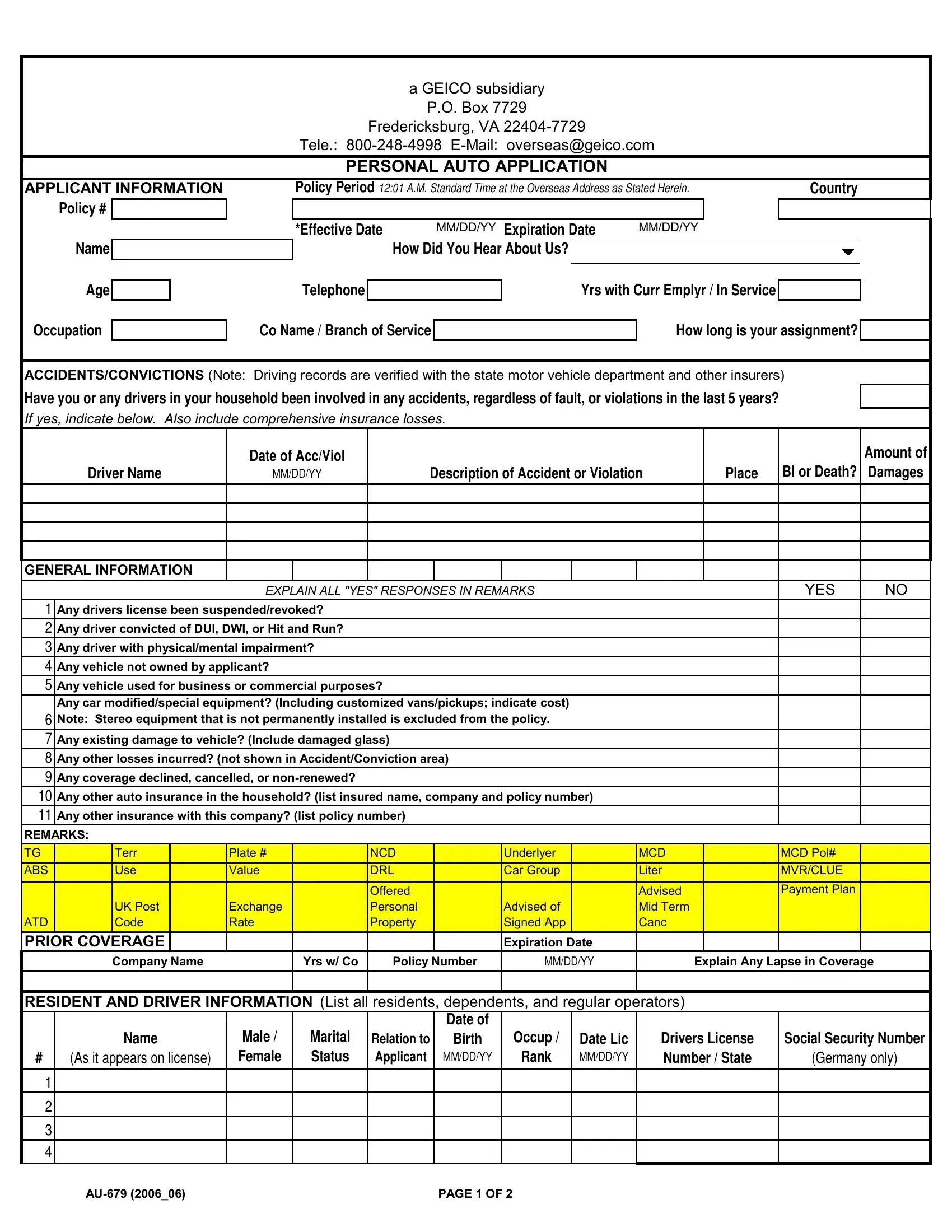
In the realm of auto insurance, the Geico AU 679 form represents a crucial document for those seeking personal auto coverage through a Geico subsidiary. Originating from Fredericksburg, VA, this form serves as a personal auto application and encapsulates a variety of information crucial for the insurance underwriting process. Applicants are required to provide comprehensive details about themselves, including personal information, vehicle data, and driving history, encompassing accidents and convictions within the past five years, to ensure accurate assessment by Geico. Key sections of the form delve into driver's license status, DUI or DWI convictions, physical or mental impairments affecting driving abilities, and the use of vehicles for business purposes. It also probes into any modifications to vehicles, existing damages, loss history, and previous insurance coverages, which collectively inform Geico’s decision-making process. The form underscores the importance of honesty in disclosures, with a clear indication that inaccuracies can lead to policy voidance. Furthermore, it outlines coverage options and premiums, stressing the policy's effective dates and the conditions under which policies can be cancelled or renewed. With spaces for applicant remarks and detailed vehicle and driver information, the AU 679 form is tailored to gather exhaustive data to facilitate a tailored insurance proposal, revealing Geico's methodical approach in offering personal auto insurance.
| Question | Answer |
|---|---|
| Form Name | Geico Form Au 679 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | geico insurance claim, why does geico require paper application, geico claim number, geico insurance claims |
a GEICO subsidiary
P.O. Box 7729
Fredericksburg, VA
Tele.:
PERSONAL AUTO APPLICATION
APPLICANT INFORMATION
Policy #
Name
Policy Period 12:01 A.M. STANDARD TIME AT THE OVERSEAS ADDRESS AS STATED HEREIN. |
|
Country |
|||||||
|
|
|
|
|
|
|
|
|
|
*Effective Date |
MM/DD/YY Expiration Date |
MM/DD/YY |
|
|
|
|
|
|
|
|
How Did You Hear About Us? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Age
Telephone
Yrs with Curr Emplyr / In Service
Occupation
Co Name / Branch of Service
How long is your assignment?
ACCIDENTS/CONVICTIONS (Note: Driving records are verified with the state motor vehicle department and other insurers)
Have you or any drivers in your household been involved in any accidents, regardless of fault, or violations in the last 5 years?
If yes, indicate below. Also include comprehensive insurance losses.
|
Date of Acc/Viol |
|
|
Amount of |
Driver Name |
MM/DD/YY |
Description of Accident or Violation |
Place |
BI or Death? Damages |
GENERAL INFORMATION
EXPLAIN ALL "YES" RESPONSES IN REMARKS |
YES |
NO |
1Any drivers license been suspended/revoked?
2Any driver convicted of DUI, DWI, or Hit and Run?
3Any driver with physical/mental impairment?
4Any vehicle not owned by applicant?
5Any vehicle used for business or commercial purposes?
Any car modified/special equipment? (Including customized vans/pickups; indicate cost)
6Note: Stereo equipment that is not permanently installed is excluded from the policy.
7Any existing damage to vehicle? (Include damaged glass)
8Any other losses incurred? (not shown in Accident/Conviction area)
9Any coverage declined, cancelled, or
10Any other auto insurance in the household? (list insured name, company and policy number)
11Any other insurance with this company? (list policy number)
REMARKS:
|
TG |
|
Terr |
|
Plate # |
|
NCD |
|
Underlyer |
|
MCD |
|
MCD Pol# |
|
|
ABS |
|
Use |
|
Value |
|
DRL |
|
Car Group |
|
Liter |
|
MVR/CLUE |
|
|
|
|
|
|
|
|
Offered |
|
|
|
Advised |
|
Payment Plan |
|
|
|
|
UK Post |
|
Exchange |
|
Personal |
|
Advised of |
|
Mid Term |
|
|
|
|
ATD |
|
Code |
|
Rate |
|
Property |
|
Signed App |
|
Canc |
|
|
|
|
PRIOR COVERAGE |
|
|
|
|
|
Expiration Date |
|
|
|
|
|||
|
|
|
Company Name |
|
Yrs w/ Co |
Policy Number |
MM/DD/YY |
Explain Any Lapse in Coverage |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RESIDENT AND DRIVER INFORMATION (List all residents, dependents, and regular operators) |
|
|
|||||||||||
|
|
|
|
|
|
|
|
Date of |
|
|
|
|
|
|
|
|
|
Name |
Male / |
Marital |
Relation to |
Birth |
Occup / |
Date Lic |
Drivers License |
Social Security Number |
|||
|
# |
(As it appears on license) |
Female |
Status |
Applicant |
MM/DD/YY |
Rank |
MM/DD/YY |
Number / State |
(Germany only) |
||||
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAGE 1 OF 2 |
|
|
|
|
|
||||
VEHICLE DESCRIPTION/USE
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
Veh Value |
|
|
|
|
|
|
|
US Spec or |
Body |
|
|
|
|
|
|
|
Purchased |
|
|
or Cost |
Year |
|
Make |
|
Model |
|
European |
Type |
|
VIN |
|
Cylinders |
|
Liters |
MM/DD/YY |
New/Used |
|
New |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of |
Miles One |
|
|
|
|
AntiLock |
|
Daytime |
Air Bags |
Sound |
|
|
|
|
|
State or Country |
|
Primary |
Way to |
|
Garaged |
|
|
|
Running |
System |
|
|||||
|
|
|
|
|
|
|
Brakes Y/N |
|
1 or 2 |
|
|||||||||
License Plate Number |
|
of Plate |
|
Driver |
Work |
|
Y / N |
Mileage |
|
Lights Y/N |
Value |
|
Act/Pass |
||||||
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
LIEN HOLDER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Addl Int |
|
Loss Payee |
Name and Address |
|
|
|
|
|
|
|
|
|
Loan Number |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONTACT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
Stateside or Home Country Address |
|
Name & Address of Nearest Relative |
|||||||||
|
Insured Location (Overseas Address) |
NOTE: COVERAGE FOR THE US IS EXCLUDED |
|
|
or Local Economy Address |
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone |
|
|
|
|
|
|
|
Telephone |
|
|
|
|
|
|
Telephone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Own / Rent |
|
|
Base |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
COVERAGES/PREMIUMS (All Amounts in USD) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Coverages |
|
|
Limits of Liability |
|
|
|
|
|
|
|
|
|
Premium |
|
|||||
Single Limit Liability (CSL) |
|
|
|
|
|
|
Ea Accident |
|
|
|
|
|
|
|
|
|
|||
Bodily Injury Liability |
|
|
|
|
|
Ea Person |
|
|
|
|
Ea Accident |
|
|
|
|
|
|||
Property Damage Liability |
|
|
|
|
Ea Accident |
|
|
|
|
|
|
|
|
|
|
||||
Medical Payments |
|
|
|
|
|
Ea Person |
|
|
|
|
|
|
|
|
|
|
|||
Comprehensive |
|
|
Ded |
|
|
ACV |
|
|
|
|
|
|
|
|
|
|
|
||
Collision |
|
|
|
|
Ded |
|
|
ACV |
|
|
|
|
|
|
|
|
|
|
|
Towing & Labor |
|
|
$100 per incident/$300 annual maximum |
|
Germany 150 Euro |
|
|
|
|
||||||||||
Rental Reimbursement |
|
$50 per day/$750 annual maximum |
|
Germany 50 or 70 Euro |
|
|
|
||||||||||||
Additional Coverages |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Ded |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ded |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Premium |
|
|
|
POLICY PERIOD |
|
|
|
|
|
|
|
|
|
|
|
|
|
Taxes |
|
|
|
||
*Effective Date |
MM/DD/YY Expiration Date |
MM/DD/YY |
|
|
|
|
|
**Total Premium |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Deposit |
|
|
|
12:01 A.M. Standard Time at the Overseas Address as Stated Above. |
|
Installments (No./Amt.) |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Installments include $5 Service Fee. Make Check Payable to "IIU". |
|||||||
*Coverage is effective the day after we receive payment and this |
|
|
|
|
|
|
|
|
$25 Charge for Returned Checks. |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
application. Not applicable if purchased in Europe. |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
**The quoted premium is subject to verification and adjustment, when necessary by the company. Policies cancelled flat are subject to a $50 processing fee. Policies cancelled prior to the expiration are subject to a minimum charge of 20% annual premium. In Belgium, Germany, Italy or Spain cancellation is permitted only for demolition, destruction, sale or export of vehicle.
I hereby warrant the truth of the above statements and declare that I have not withheld any information whatever which might tend to influence the acceptance of this application. I understand that any false statement by me will constitute a breach of warranty and cause the policy to be void. I agree that this application shall be the basis of the Policy between me and the Company(s). I understand that my policy will be automatically renewed if I do not state otherwise. We reserve the right to review the applicants information along with information developed on any investigative reports, to determine eligibility for insurance.
|
|
|
|
|
IIU / Agt Code |
X |
|
|
X |
|
Producer Code |
Applicant's Signature |
Date |
|
Agent's Signature |
Date |
|
MM/DD/YY |
|
MM/DD/YY |
|||
|
|
|
|||
PAGE 2 OF 2 |