
Whenever you would like to fill out sar 7 form san bernardino county, you won't have to download any sort of programs - simply try using our PDF tool. Our team is continuously working to improve the tool and enable it to be even faster for clients with its extensive features. Unlock an ceaselessly progressive experience now - check out and uncover new possibilities as you go! All it requires is a couple of easy steps:
Step 1: Hit the orange "Get Form" button above. It is going to open our pdf tool so you could begin completing your form.
Step 2: With the help of this state-of-the-art PDF tool, you can actually accomplish more than just complete blank form fields. Edit away and make your forms seem great with custom textual content added, or optimize the original content to perfection - all that accompanied by an ability to insert your own pictures and sign the document off.
It's straightforward to complete the pdf following this practical tutorial! Here is what you need to do:
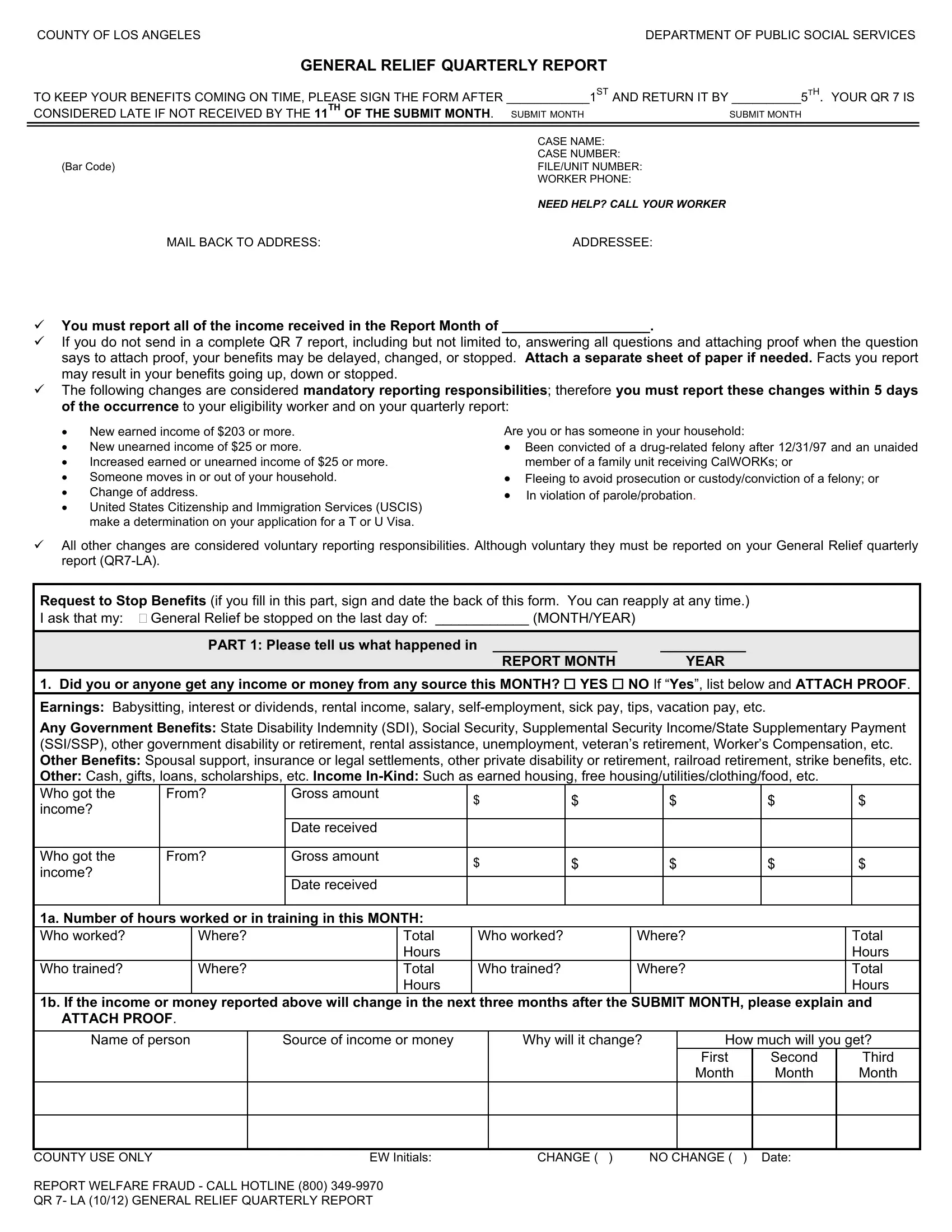
1. First of all, when filling in the sar 7 form san bernardino county, begin with the area that features the subsequent fields:
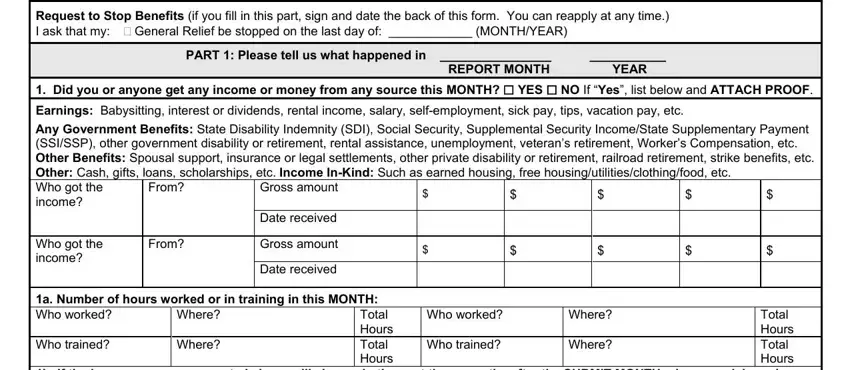
2. After finishing the last part, go on to the subsequent step and enter the necessary particulars in these fields - Request to Stop Benefits if you, PART Please tell us what happened, REPORT MONTH YEAR, Did you or anyone get any income, Earnings Babysitting interest or, Any Government Benefits State, Gross amount, From, Who got the income, Date received, From, Gross amount, Date received, Total Hours Total Hours, and a Number of hours worked or in.
3. Throughout this stage, examine COUNTY USE ONLY REPORT WELFARE, EW Initials, First Month, Second Month, Third Month, CHANGE, and NO CHANGE Date. All these have to be filled in with greatest focus on detail.

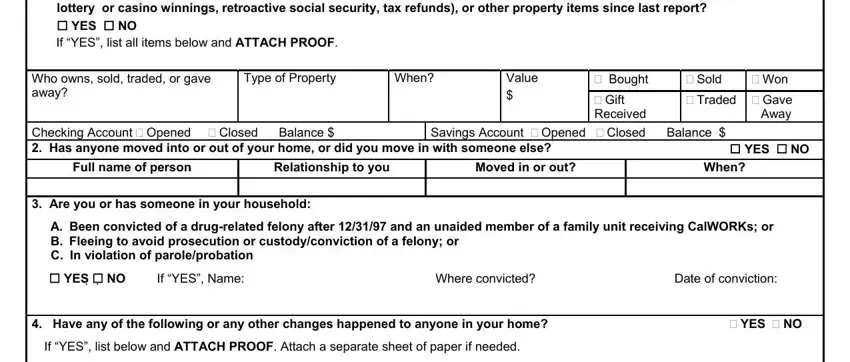
4. This specific part arrives with these empty form fields to complete: Did anyone Get buy sell trade or, lottery or casino winnings, cid YES cid NO If YES list all, Type of Property, Value, When, Bought Gift Received, Sold Traded Gave, Won, Away, Savings Account Opened Closed, cid YES cid NO, Full name of person, Relationship to you, and Moved in or out.
5. The last notch to complete this form is crucial. Ensure you fill in the mandatory form fields, and this includes Family Change Married divorced, DP became pregnant had a baby or, Disability Became disabled or, strike, Immigration Citizenship or, Name of person s, Relationship to you, What happened, Date of change, ADDRESS CHANGE, Fill in this section ONLY if you, NEW Home Address Number Street, NEW Mailing Address if different, New Phone Number, and Do you have housing costs at this, before using the form. Failing to accomplish that can end up in a flawed and possibly invalid form!
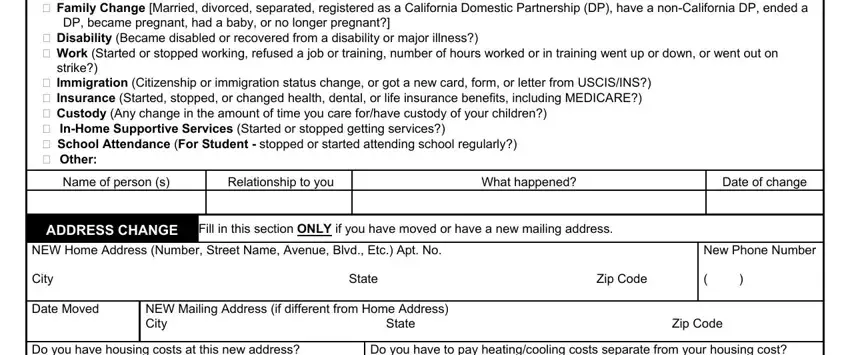
As to Date of change and ADDRESS CHANGE, be certain that you do everything properly in this section. The two of these are certainly the most significant fields in the PDF.
Step 3: Reread the information you've entered into the blanks and then click on the "Done" button. Join FormsPal right now and immediately get sar 7 form san bernardino county, prepared for downloading. All adjustments made by you are preserved , allowing you to edit the form at a later time if needed. FormsPal guarantees risk-free document completion without personal data record-keeping or distributing. Be assured that your details are secure with us!