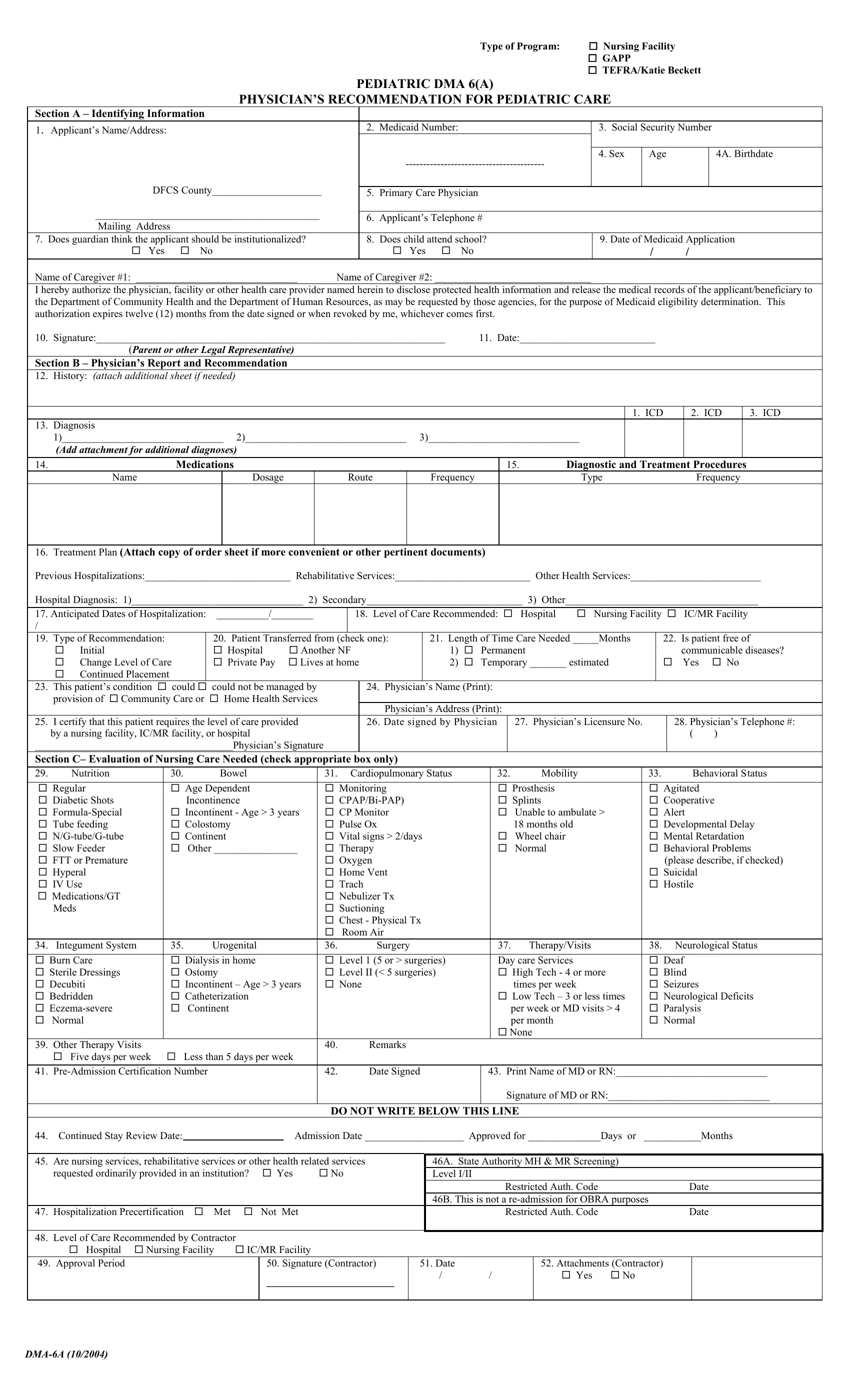

Facility or administrative staff may complete Section A (Identifying Information). The physician completes and signs Sections B and C. You can complete the Georgia DMA-6 form in our PDF editor or download the file to your device. Then, follow the steps below.
1. Identifying Information
Begin by entering the patient’s basic details, including full name, address, Medicaid number, Social Security number, date of birth, sex, and county.
Then, select the type of facility being requested and the reason for the submission, such as an initial placement or continued stay. Include the patient’s current location and the expected admission date.
2. Physician’s Examination and Recommendation
The physician completes this section, documenting the patient’s medical condition and care needs. This includes the primary and secondary diagnoses, ICD codes (when available), and a summary of the patient’s medical history, current condition, and recent hospitalizations.
The medications should be listed with their dosages and frequency, along with any diagnostic tests or treatment procedures.
The form also requires an indication of whether the need for care is temporary or long term, as well as an estimate of how long services will be needed.
3. Evaluation of Nursing Care Needed
Check the boxes that best describe the patient’s current condition. This section covers nutrition, bowel and bladder function, mobility, behavior, cognitive status, therapies, impairments, and activities of daily living.
Base each selection on how the patient functions on a typical day, not on occasional improvements or best-case days.
4. Physician Certification and Signatures
At the end of the form, the physician signs and dates the document and provides license and contact information.
Do not complete any section marked “Do Not Write Below This Line,” as Medicaid reviewers use those areas during the authorization process.