The Georgia 5579 form plays a crucial role in safeguarding the welfare of children in residential care settings, facilitating a thorough vetting process for individuals seeking to work within such environments. Administered by the Georgia Department of Human Resources, this form serves as a Residential Child Care Records Check Application, meticulously designed to compile comprehensive personal and professional information from applicants. Essential for directors, managers, owners, and employees with a criminal history seeking roles in residential child care, the form necessitates detailed inputs ranging from personal identification to authorization for conducting criminal history checks. Besides personal identification details such as name, date of birth, and Social Security number, applicants are required to disclose any past arrests, charges, or convictions, with exceptions limited to mere parking violations. This comprehensive process underscores the rigor with which Georgia scrutinizes potential care providers, ensuring that only those with unblemished records and genuine intent can contribute to the nurturing and safe environments critical for children in residential care. Such meticulous checks are vital, given the sensitive nature of the work and the vulnerability of the children involved, showcasing the state's commitment to child welfare through stringent regulatory measures.
| Question | Answer |
|---|---|
| Form Name | Georgia Form 5579 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Peachtree, OIS, sample motion for reconsideration georgia, motion to reconsider the family law order form |
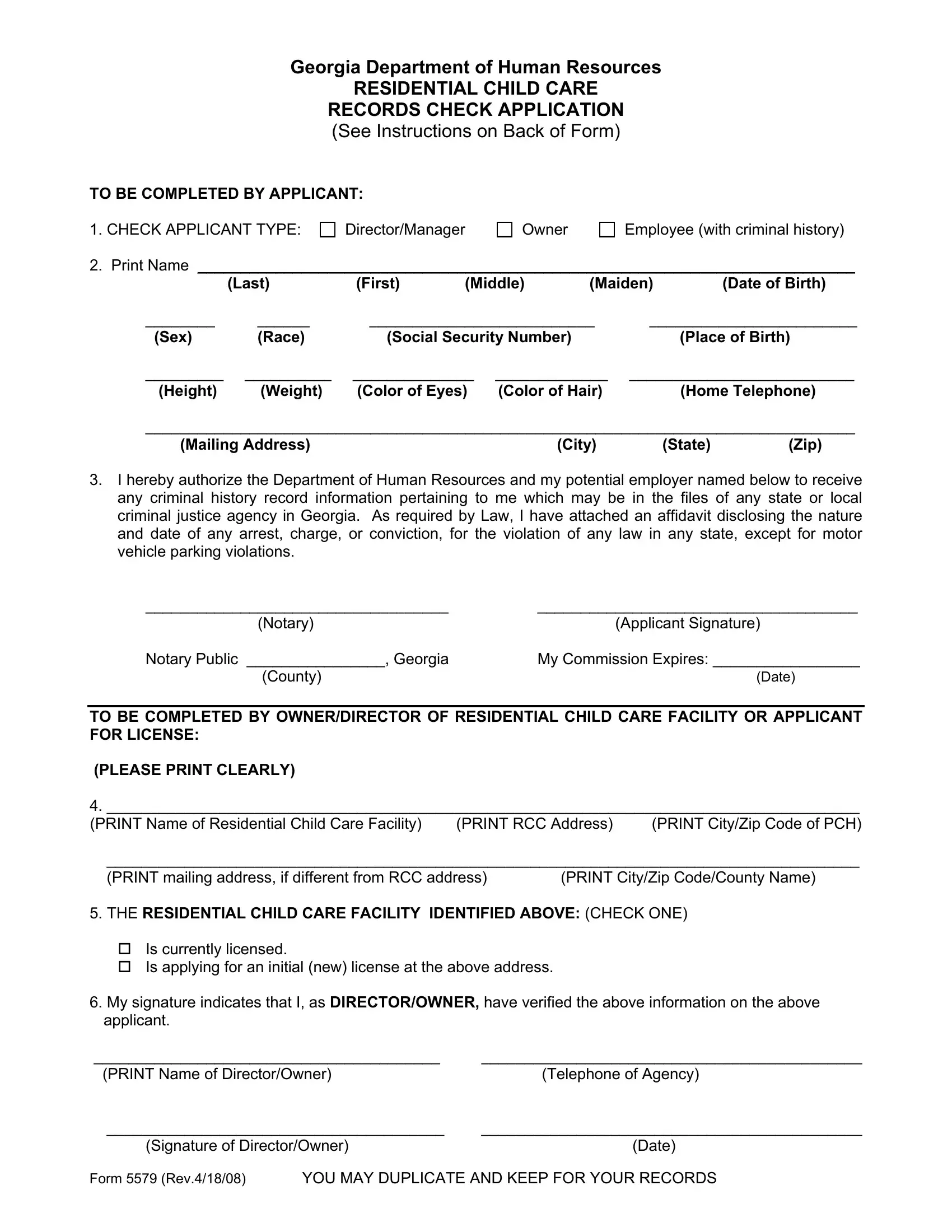
Georgia Department of Human Resources
RESIDENTIAL CHILD CARE
RECORDS CHECK APPLICATION (See Instructions on Back of Form)
TO BE COMPLETED BY APPLICANT:
1. CHECK APPLICANT TYPE: |
Director/Manager |
Owner
Employee (with criminal history)
2.Print Name ____________________________________________________________________________
|
(Last) |
(First) |
(Middle) |
(Maiden) |
(Date of Birth) |
|
________ |
______ |
__________________________ |
________________________ |
|||
(Sex) |
(Race) |
(Social Security Number) |
|
|
(Place of Birth) |
|
_________ __________ ______________ _____________ __________________________
(Height) (Weight) (Color of Eyes) (Color of Hair) (Home Telephone)
__________________________________________________________________________________
(Mailing Address) |
(City) |
(State) |
(Zip) |
3.I hereby authorize the Department of Human Resources and my potential employer named below to receive any criminal history record information pertaining to me which may be in the files of any state or local criminal justice agency in Georgia. As required by Law, I have attached an affidavit disclosing the nature and date of any arrest, charge, or conviction, for the violation of any law in any state, except for motor vehicle parking violations.
___________________________________ |
_____________________________________ |
(Notary) |
(Applicant Signature) |
Notary Public ________________, Georgia |
My Commission Expires: _________________ |
(County) |
(Date) |
TO BE COMPLETED BY OWNER/DIRECTOR OF RESIDENTIAL CHILD CARE FACILITY OR APPLICANT FOR LICENSE:
(PLEASE PRINT CLEARLY)
4. _______________________________________________________________________________________
(PRINT Name of Residential Child Care Facility) (PRINT RCC Address) (PRINT City/Zip Code of PCH)
_______________________________________________________________________________________
(PRINT mailing address, if different from RCC address) |
(PRINT City/Zip Code/County Name) |
5.THE RESIDENTIAL CHILD CARE FACILITY IDENTIFIED ABOVE: (CHECK ONE)
Is currently licensed.
Is applying for an initial (new) license at the above address.
6.My signature indicates that I, as DIRECTOR/OWNER, have verified the above information on the above applicant.
________________________________________ |
____________________________________________ |
(PRINT Name of Director/Owner) |
(Telephone of Agency) |
_______________________________________ |
____________________________________________ |
(Signature of Director/Owner) |
(Date) |
Form 5579 (Rev.4/18/08) YOU MAY DUPLICATE AND KEEP FOR YOUR RECORDS

Application Instructions
Do not have the Live Scan done before turning in your application package.
1.Please use a ball point pen, press firmly, and PRINT legibly.
2.Please indicate if you are a director/ manager, an owner or an employee (with a criminal history). You should check both owner and director/manager if you are both the administrator and the owner.
3.Print your full name, including your MAIDEN name. DO NOT use initials if your have a given name.
Print your date of birth. Print either: Male or Female.
Print your race: Black, White, or Other. Print your Social Security Number.
Print your place of birth: City or County, State and Country if not USA. Print your height.
Print your weight.
Print the color of your eyes: Do NOT abbreviate: Brown, Black, Grey, Blue, Green, or Hazel.
Print the color of your hair: DO NOT abbreviate: Brown, Black, Grey, Red, Blonde, or Bald. Print your home address.
Print your home telephone number.
4.ALL APPLICATIONS MUST BE NOTARIZED. Read the consent statement.
Sign your name as you would on a bank check or business letter.
DIRECTOR/OWNER WILL COMPLETE THE FOLLOWING
5.Record check results will be mailed to the address that is entered here. Print clearly and give complete mailing address.
Indicate name of your facility as it appears on your permit or permit application. Print the address of the Residential Child Care Facility.
Print the mailing address where the letter of determination is to be sent. Print the city/zip/county.
6.Check the correct box to indicate current licensure status for your Residential Child Care facility.
7.Director or Owner must sign his/her name as it would appear on a bank check or business letter.
8.This form must be completed and brought with you for Live Scans at 2 Peachtree or specified
Office of Investigative Services
Background Investigations Unit
2 Peachtree Street, N.W., Suite 30.482
Atlanta, GA.
9.If the Criminal Records Check Application is not received by OIS, you will not receive a determination letter.
10.This form should be sent to OIS before the fingerprinting at the COGENT/GAPS location is done.