


Once you open the online tool for PDF editing by FormsPal, you can fill in or alter how to ga form medicaid right here and now. To make our editor better and simpler to use, we continuously design new features, considering feedback coming from our users. If you're seeking to get started, here is what it's going to take:
Step 1: Access the PDF in our tool by clicking on the "Get Form Button" in the top part of this webpage.
Step 2: The editor allows you to change your PDF form in a range of ways. Enhance it by including customized text, correct original content, and place in a signature - all doable within a few minutes!
This document requires specific information; in order to guarantee correctness, you should bear in mind the following suggestions:
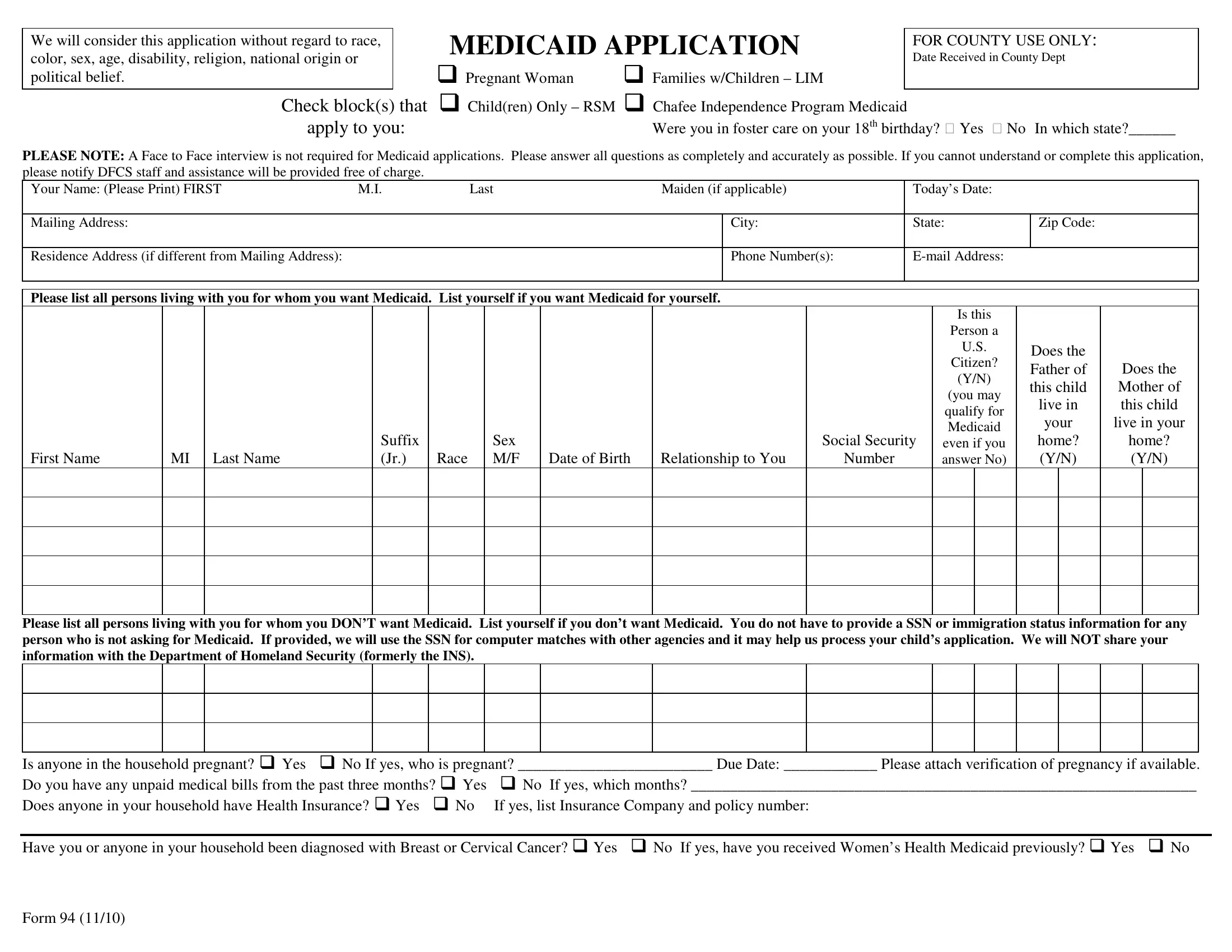
1. You'll want to complete the how to ga form medicaid properly, therefore be attentive when filling out the segments that contain all of these blanks:
2. Right after finishing the previous step, go on to the next step and complete the necessary particulars in these blanks - First Name, Please list all persons living, Is anyone in the household, and Form.

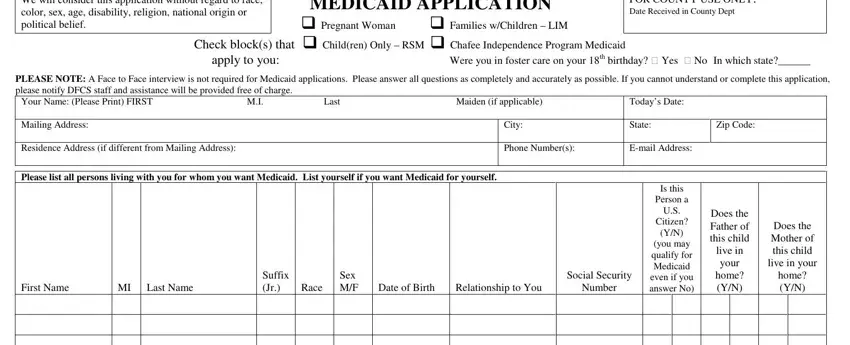
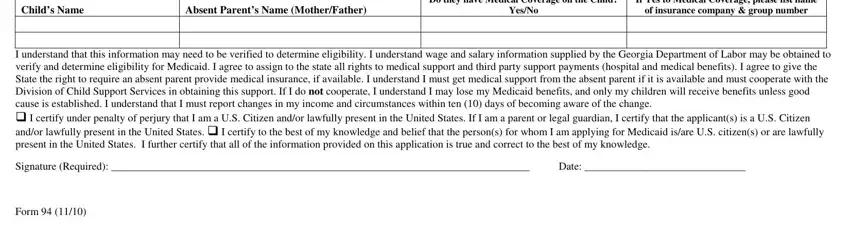
3. This next part will be about Check, weekly every weeks, Income, WagesEarnings, amount before deductions, Current Employer, WagesEarnings, Current Employer, monthly etc, Name of Person Receiving, Resources Cash, Checking Account Savings Account, Social Security IncomeSSI Workers, KRetirement Account Other, and Model - fill out all of these blanks.
People generally make errors when completing Check in this area. Don't forget to revise whatever you enter right here.
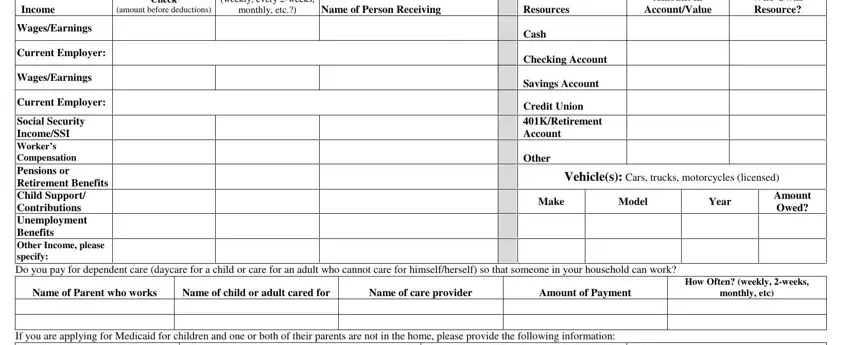
4. The next section comes next with the next few fields to fill out: If you are applying for Medicaid, Childs Name, Absent Parents Name MotherFather, YesNo, If Yes to Medical Coverage please, of insurance company group number, I understand that this information, Date, and Form.
Step 3: After you have glanced through the information entered, press "Done" to finalize your document generation. Create a free trial account with us and gain instant access to how to ga form medicaid - download, email, or edit inside your FormsPal account page. When you work with FormsPal, you're able to fill out documents without stressing about database incidents or data entries getting shared. Our secure system ensures that your private information is stored safely.