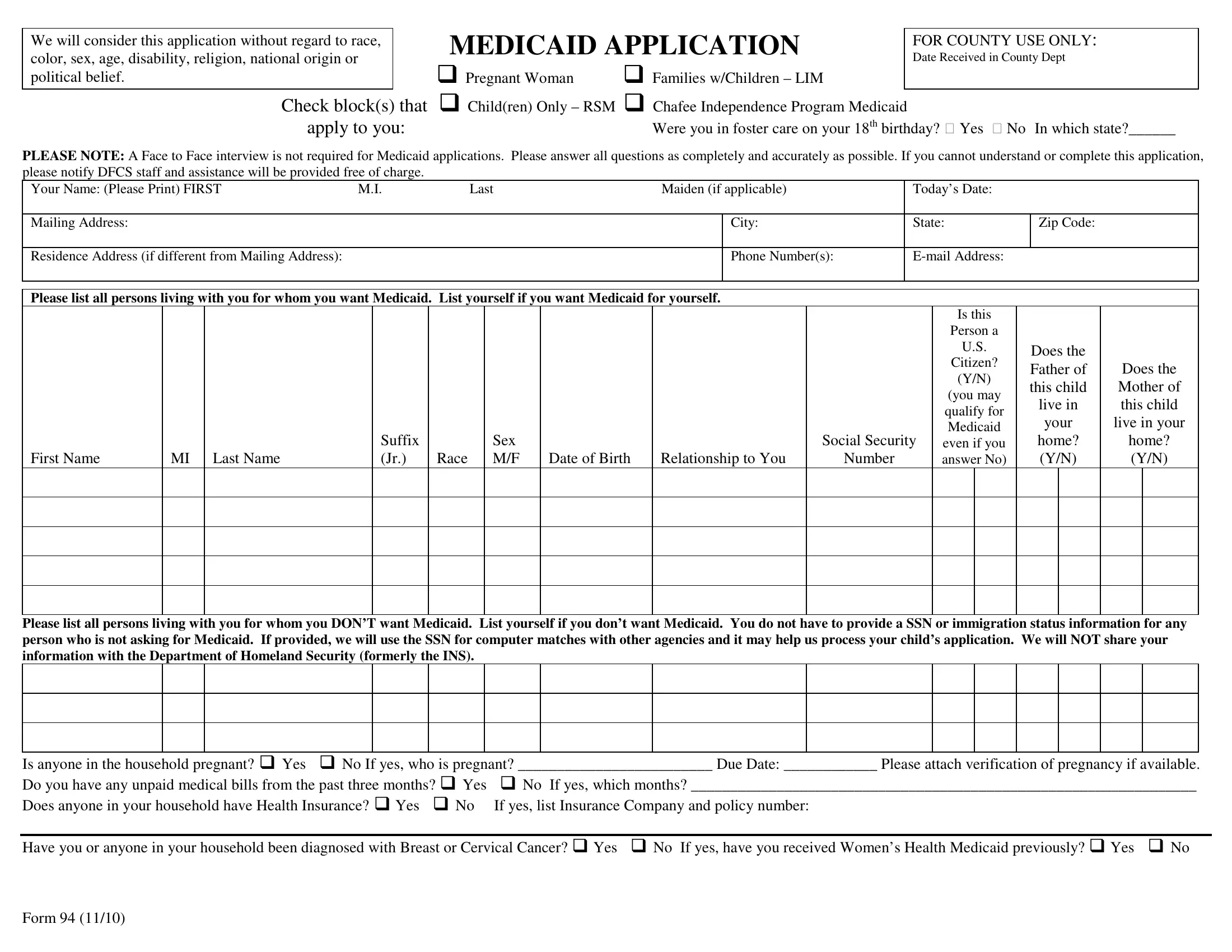
The Georgia Medicaid Application form is a critical step for residents in Georgia who are seeking health coverage through the state’s Medicaid program. This comprehensive form is designed to gather all necessary information to evaluate an individual’s eligibility for Medicaid, without discrimination based on race, color, sex, age, disability, religion, national origin, or political belief. Applicants are urged to provide detailed information regarding their living situation, including but not limited to the number of individuals living in their household who are seeking Medicaid, citizenship status, and the presence of any pregnant women. It also inquires about current health insurance coverage, recent diagnoses of serious conditions such as Breast or Cervical Cancer, and any unpaid medical bills from the past three months, signaling its thoroughness in assessing applicants' needs. Additionally, the form requests details about income, resources, and any dependent care expenses to determine financial eligibility. Importantly, the Georgia Medicaid Application points out that a face-to-face interview is not required, thereby streamlining the process. Nevertheless, for those who find the form challenging, assistance is offered through the Department of Family and Children Services (DFCS) to ensure that no one is barred from applying due to the complexity of the form. Completing this form accurately is paramount, as it includes a declaration under penalty of perjury regarding the applicant’s citizenship status and the accuracy of the information provided. Highlighting a commitment to fair and efficient processing, this form plays a pivotal role in connecting Georgia residents with valuable Medicaid benefits.
| Question | Answer |
|---|---|
| Form Name | Georgia Form Medicaid Application |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | online application for medicaid in georgia, medicaid forms georgia, medicaid forms ga, medicaid application form georgia |