
georgia form sbwc can be filled out online effortlessly. Just make use of FormsPal PDF editor to get it done in a timely fashion. FormsPal development team is continuously working to develop the tool and make it much easier for clients with its multiple functions. Make the most of today's innovative prospects, and find a heap of new experiences! Should you be looking to begin, this is what it takes:
Step 1: Just click on the "Get Form Button" above on this site to launch our pdf editing tool. Here you will find all that is required to work with your document.
Step 2: The editor will allow you to change PDF files in a variety of ways. Transform it by adding personalized text, adjust what is already in the PDF, and add a signature - all within a few clicks!
Pay attention while completing this form. Make sure every single blank is completed accurately.
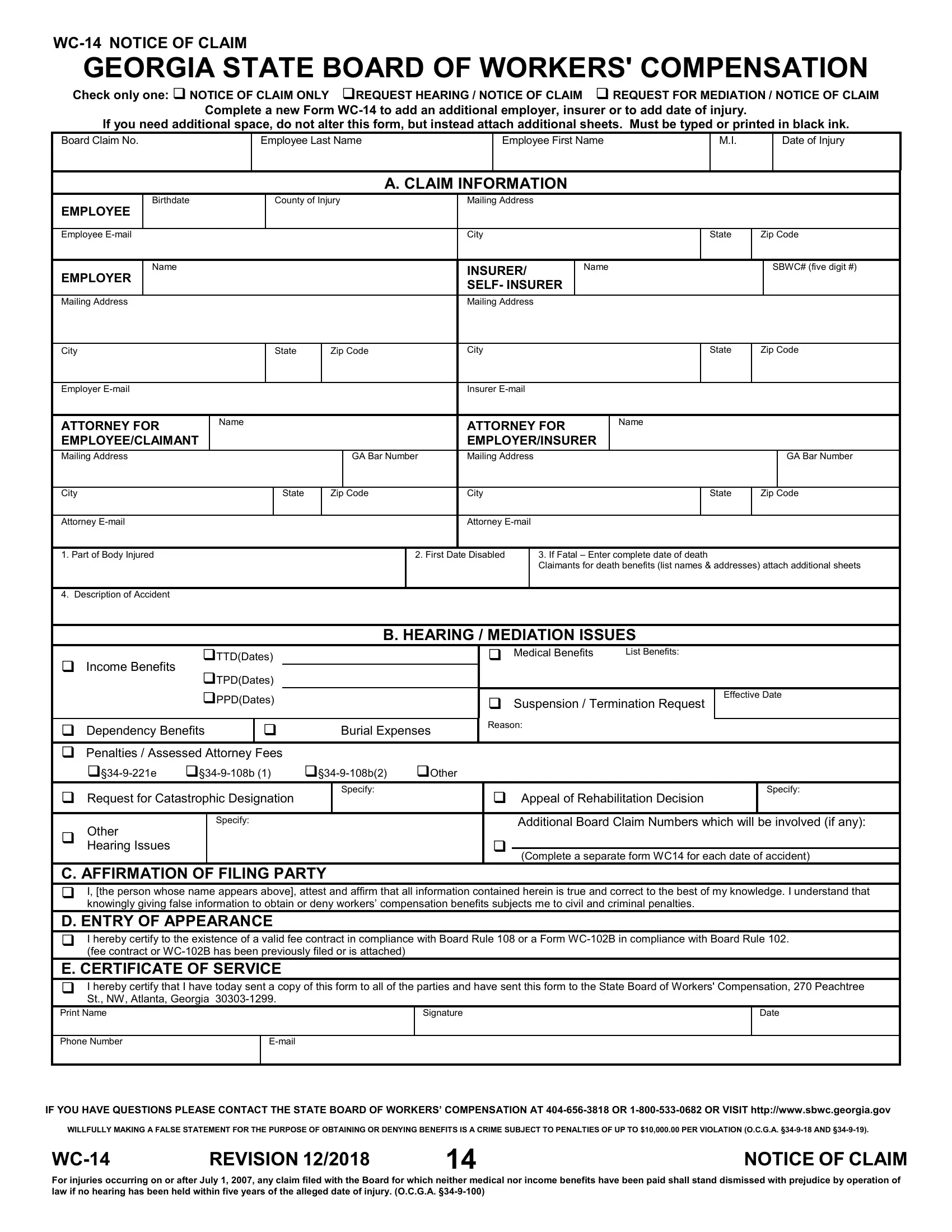
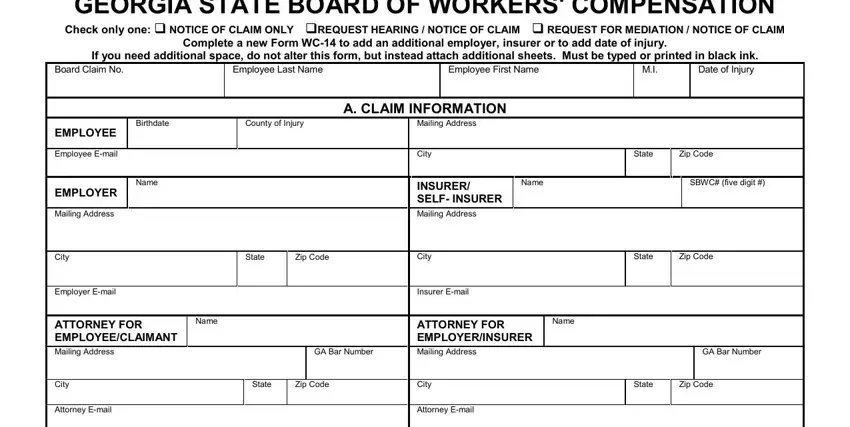
1. First, when filling in the georgia form sbwc, beging with the area that includes the following blank fields:
2. Just after filling in the last part, go to the next stage and fill out all required particulars in these blanks - First Date Disabled, If Fatal Enter complete date of, B HEARING MEDIATION ISSUES, Medical Benefits, List Benefits, Suspension Termination Request, Effective Date, City Attorney Email Part of Body, Description of Accident, Income Benefits, TTDDates TPDDates PPDDates, Dependency Benefits Penalties, Request for Catastrophic, Other Hearing Issues, and Specify.
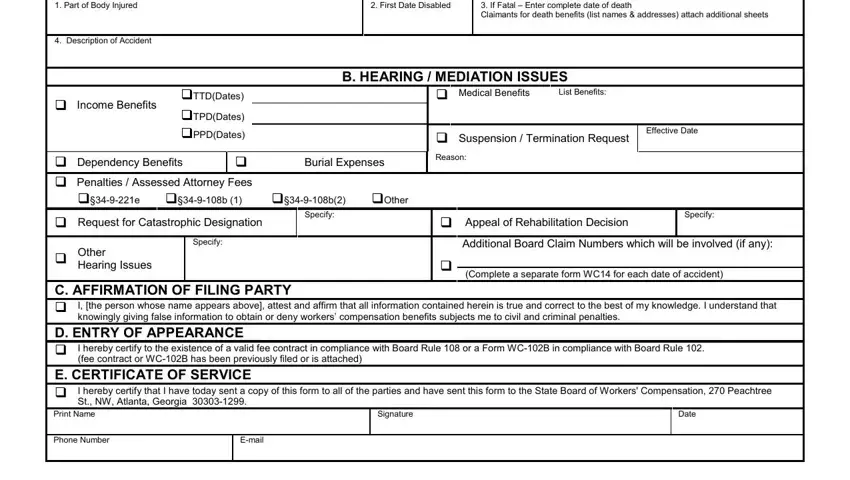
People often get some points incorrect while filling out Dependency Benefits Penalties in this area. Be sure you double-check everything you enter right here.
Step 3: Proofread all the details you have inserted in the form fields and hit the "Done" button. Sign up with FormsPal right now and easily get access to georgia form sbwc, all set for downloading. Every single change made is handily preserved , making it possible to change the form at a later time as needed. FormsPal guarantees your information privacy by having a protected system that in no way records or shares any sort of sensitive information used in the form. You can relax knowing your paperwork are kept confidential any time you work with our service!