
With the help of the online PDF editor by FormsPal, you'll be able to complete or modify green shield canada forms right here. FormsPal expert team is constantly working to develop the editor and insure that it is much easier for people with its cutting-edge features. Enjoy an ever-improving experience now! Starting is effortless! All you need to do is adhere to these basic steps down below:
Step 1: Open the PDF in our tool by hitting the "Get Form Button" in the top section of this page.
Step 2: With our handy PDF editing tool, you may accomplish more than just fill out blank fields. Express yourself and make your forms appear professional with custom text added, or adjust the original input to perfection - all comes with the capability to insert stunning photos and sign it off.
Concentrate when filling out this document. Make sure all required blanks are filled out accurately.
1. Firstly, while filling out the green shield canada forms, begin with the form section that has the next blank fields:
2. Given that the previous part is finished, you're ready insert the essential specifics in TOTAL CLAIMED, FOR PRESCRIPTION DRUG CLAIMS ONLY, TO FACILITATE CLAIMS PROCESSING, Please note Cash register, DIN, If injectable please provide, If claim is from OUT OF COUNTRY, Name of Country Visited Currency, SIGNATURE OF PLAN MEMBER, DATE, By signing this claim form and, I am authorized by my spouse andor, and SECTION MAILING INSTRUCTIONS See so you're able to move on further.
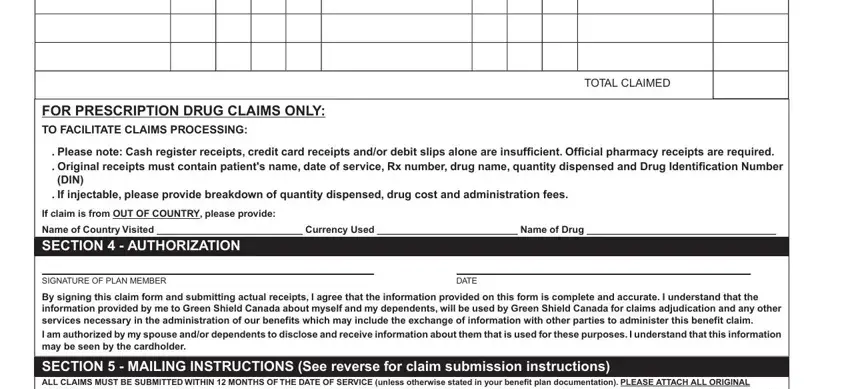
Concerning Name of Country Visited Currency and TOTAL CLAIMED, make sure you get them right here. These could be the most important ones in the document.
Step 3: Immediately after taking one more look at your entries, hit "Done" and you're good to go! Join FormsPal now and instantly use green shield canada forms, prepared for download. All changes you make are preserved , letting you modify the file at a later time if necessary. Here at FormsPal, we aim to make sure that your information is maintained protected.