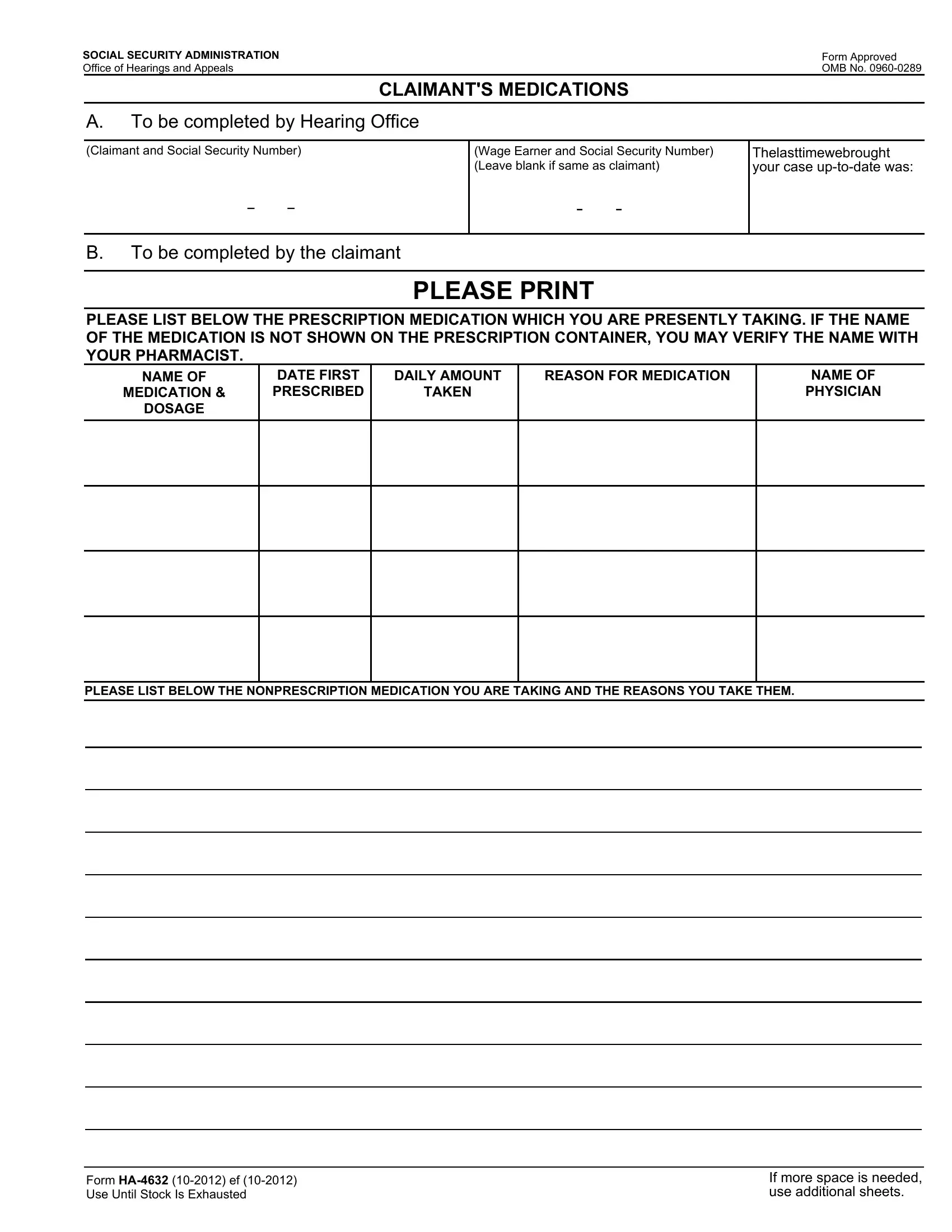
Navigating the complexities of the Social Security Administration's procedures, the HA-4632 form plays a crucial role for those undergoing the appeal process regarding their Social Security benefits. Designed to be completed by claimants, this document meticulously records the prescribed and nonprescription medications that an individual is taking. Accuracy and thoroughness are paramount, as the information provided helps evaluate an individual's health condition in relation to their claim. The form itself is divided into sections that request detailed information about each medication, including its name, the date it was first prescribed, the daily dosage, and the reasoning behind taking it, emphasizing the need for claimants to collaborate with their healthcare providers to ensure accuracy. Furthermore, the form serves a broader purpose, going beyond just collecting medication information. It is part of a larger system aimed at maintaining the integrity of Social Security programs, with provisions for information sharing under certain conditions to assist in benefit determination, compliance with federal laws, and eligibility evaluations for similar programs. The importance of submitting this form when requested cannot be overstated, as failure to provide the requested information may impact the re-evaluation of a claim. Recognizing the balance between the need for personal information and privacy, the Social Security Administration outlines specific routine uses for the data collected and emphasizes the voluntary nature of this information provision. Compliant with the Paperwork Reduction Act, the form reflects the administration's effort to streamline the information collection process while ensuring that claimants understand their rights and the implications of their participation.
| Question | Answer |
|---|---|
| Form Name | Ha 4632 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | claimant form download, ssa ha, social claimant, social security ha 4632 |
SOCIAL SECURITY ADMINISTRATION |
|
|
Form Approved |
|
Office of Hearings and Appeals |
|
|
OMB No. |
|
|
|
CLAIMANT'S MEDICATIONS |
|
|
|
|
|
|
|
A. |
To be completed by Hearing Office |
|
||
|
|
|
|
|
(Claimant and Social Security Number) |
|
(Wage Earner and Social Security Number) |
Thelasttimewebrought |
|
|
|
|
(Leave blank if same as claimant) |
your case |
|
- - |
|
- - |
|
|
|
|
|
|
B. |
To be completed by the claimant |
|
||
|
|
|
|
|
|
|
PLEASE PRINT |
|
|
PLEASE LIST BELOW THE PRESCRIPTION MEDICATION WHICH YOU ARE PRESENTLY TAKING. IF THE NAME OF THE MEDICATION IS NOT SHOWN ON THE PRESCRIPTION CONTAINER, YOU MAY VERIFY THE NAME WITH YOUR PHARMACIST.
NAME OF |
DATE FIRST |
DAILY AMOUNT |
REASON FOR MEDICATION |
NAME OF |
MEDICATION & |
PRESCRIBED |
TAKEN |
|
PHYSICIAN |
DOSAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE LIST BELOW THE NONPRESCRIPTION MEDICATION YOU ARE TAKING AND THE REASONS YOU TAKE THEM.
Form
If more space is needed, use additional sheets.
Privacy Act Statement Collection and Use
of Personal Information
Sections 205, 1631(d)(1), and 1872 of the Social Security Act, as amended authorize us to collect this information. We will use this information to evaluate your reason for failing to appear at your scheduled hearing.
Furnishing us this information is voluntary. However, failing to provide us with all or part of the requested information may affect our ability to
We rarely use the information you supply for any purpose other than for determining problems in Social Security programs. However, we may use it for the administration and integrity of Social Security programs. We may also disclose information to another person or to another agency in accordance with approved routine uses, which include, but are not limited to the following:
1.To enable a third party or an agency to assist Social Security in establishing rights to Social Security benefits and/or coverage;
2.To comply with Federal Laws requiring the release of information from Social Security records (e.g., to the Government Accountability Office and the Department of Veterans’Affairs);
3.To make determinations for eligibility in similar health and income maintenance programs as at the Federal, State, and local level; and
4.To facilitate statistical research, audit, or investigative activities necessary to assure the integrity of Social Security programs.
We may also use the information you provide in computer matching programs. Matching programs compare our records with records kept by other Federal, State, or local government agencies. Information from these matching programs can be used to establish or verify a person’s eligibility for
A complete use of routine uses for this information is available in our Systems of Records Notices,
Paperwork Reduction Act Statement - This information collection meets the requirements of 44 U.S.C. § 3507, as amended by Section 2 of the Paperwork Reduction Act of 1995. You do not need to answer these questions unless we display a valid Office of Management and Budget control number. We estimate that it will take about 15 minutes to read the instructions, gather the facts, and answer the questions. You may send comments on our time estimate above to: SSA, 6401 Security Blvd., Baltimore, MD
Form