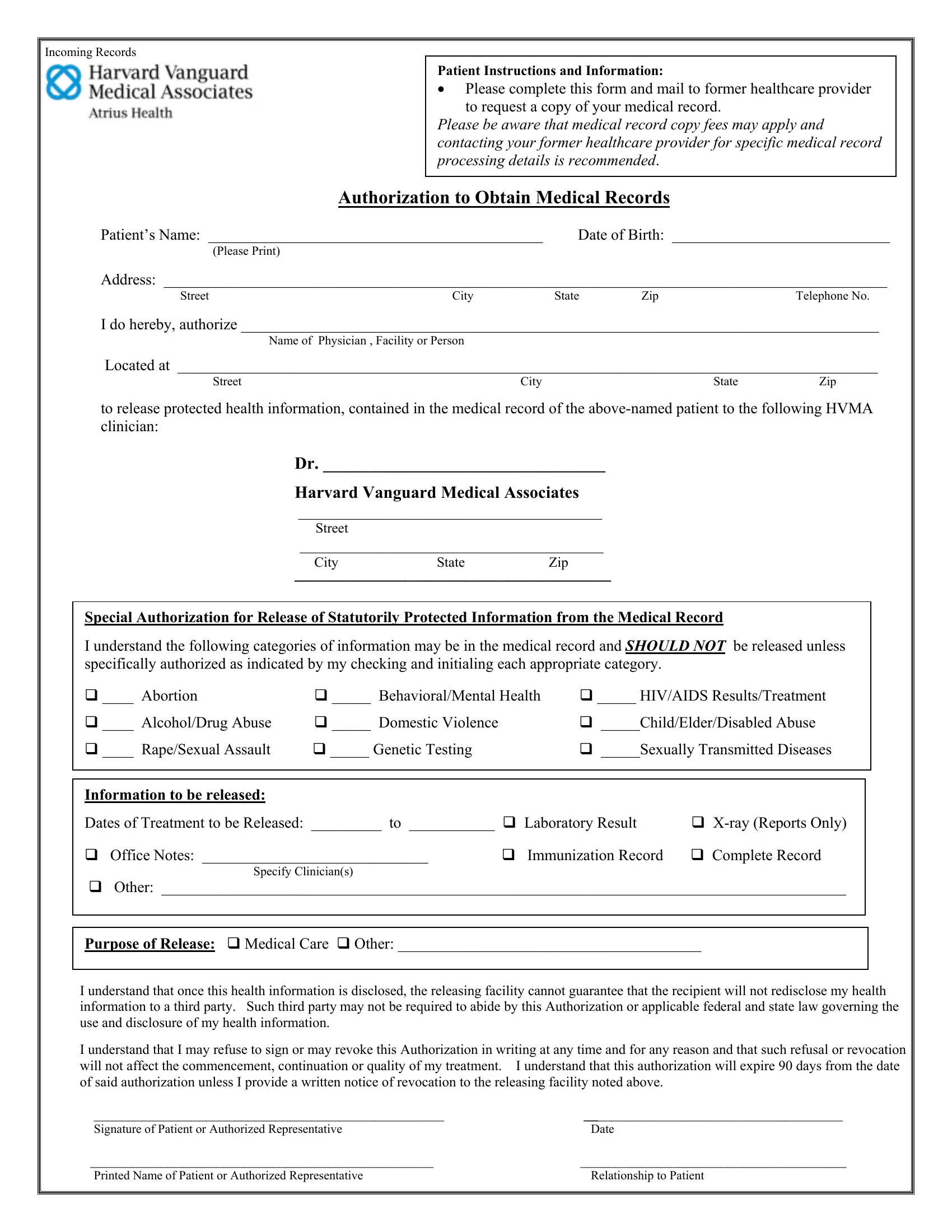
When patients find themselves transitioning to Harvard Vanguard Medical Associates (HVMA) for their healthcare needs, a crucial step involves obtaining and transferring their medical records. The Harvard Vanguard Records Form serves as a patient's authorization to facilitate this important process. This form is a comprehensive document that patients complete and send to their former healthcare providers, authorizing the release of their medical records to their designated HVMA clinician. It covers the transfer of varied medical information, including laboratory results, X-rays, office notes, immunization records, and more. Patients are instructed to provide detailed personal information, the specific dates of treatment for which records are needed, and to specify the type of medical information to be released. Notably, the form addresses the release of highly sensitive information, such as mental health records, genetic testing results, and sexual health information, requiring patients to give explicit authorization for these categories by initialing them. Additionally, the form enlightens patients about potential fees, the finite nature of the authorization period, and the importance of contacting their former healthcare provider for specifics on the medical record processing. Lastly, it ensures patients are aware that once their health information is disclosed, the responsibility for the privacy of that information may no longer rest with the releasing facility, highlighting the significance of informed consent in the medical records transfer process.
| Question | Answer |
|---|---|
| Form Name | Harvard Vanguard Records Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | hvma medical records, harvard vanguard medical records department, harvard vanguard medical records, harvard vanguard wellesley medical records phone number |
Incoming Records
Patient Instructions and Information:
•Please complete this form and mail to former healthcare provider to request a copy of your medical record.
Please be aware that medical record copy fees may apply and contacting your former healthcare provider for specific medical record processing details is recommended.
Authorization to Obtain Medical Records
Patient’s Name: ___________________________________________ |
Date of Birth: ____________________________ |
(Please Print) |
|
Address: _____________________________________________________________________________________________
StreetCity State ZipTelephone No.
I do hereby, authorize __________________________________________________________________________________
Name of Physician , Facility or Person
Located at __________________________________________________________________________________________
Street |
City |
State |
Zip |
to release protected health information, contained in the medical record of the
Dr. _________________________________
Harvard Vanguard Medical Associates
_______________________________________
Street
_______________________________________
CityState Zip
_____________________________________
Special Authorization for Release of Statutorily Protected Information from the Medical Record
I understand the following categories of information may be in the medical record and SHOULD NOT be released unless specifically authorized as indicated by my checking and initialing each appropriate category.
____ Abortion |
_____ Behavioral/Mental Health |
_____ HIV/AIDS Results/Treatment |
|
||
____ Alcohol/Drug Abuse |
_____ Domestic Violence |
|
_____Child/Elder/Disabled Abuse |
|
|
____ Rape/Sexual Assault |
_____ Genetic Testing |
|
_____Sexually Transmitted Diseases |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Information to be released: |
|
|
|
|
|
Dates of Treatment to be Released: _________ to ___________ |
Laboratory Result |
|
|||
Office Notes: _____________________________ |
Immunization Record |
Complete Record |
|
||
Specify Clinician(s) |
|
|
|
|
|
Other: ________________________________________________________________________________________
Purpose of Release: |
Medical Care |
Other: _______________________________________ |
I understand that once this health information is disclosed, the releasing facility cannot guarantee that the recipient will not redisclose my health information to a third party. Such third party may not be required to abide by this Authorization or applicable federal and state law governing the use and disclosure of my health information.
I understand that I may refuse to sign or may revoke this Authorization in writing at any time and for any reason and that such refusal or revocation will not affect the commencement, continuation or quality of my treatment. I understand that this authorization will expire 90 days from the date of said authorization unless I provide a written notice of revocation to the releasing facility noted above.
__________________________________________________ |
_____________________________________ |
Signature of Patient or Authorized Representative |
Date |
_________________________________________________ |
______________________________________ |
Printed Name of Patient or Authorized Representative |
Relationship to Patient |
|
|