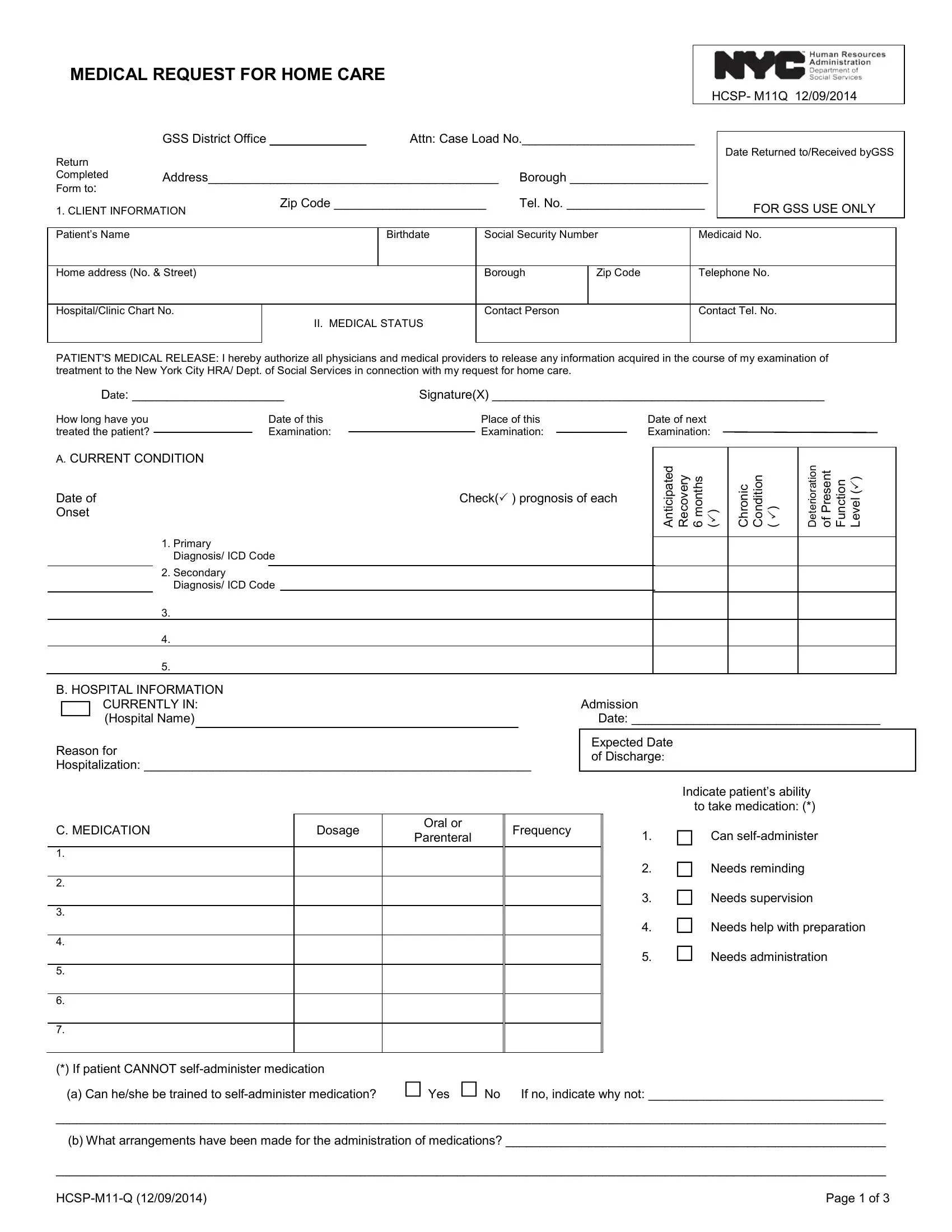
The HCSP-M11Q form, also known as the Medical Request for Home Care, serves as a crucial document in the process of acquiring home care services for individuals necessitating medical assistance in their residences. Dated December 9, 2014, and intended for submission to the GSS District Office, this comprehensive form captures essential client information, including personal and contact details, alongside a detailed medical status that requires a physician's certification. The form facilitates the authorization for physicians to release medical information to the New York City HRA/Dept. of Social Services, aiming to streamline the patient's request for home care. It encompasses sections on the patient's current condition, medication regimen, hospital information, and the medical treatments received or needed, which collectively paint a clear picture of the patient's health needs. Furthermore, it probes into the patient’s ability to manage medication, the necessity for personal care and/or housekeeping assistance, the requirement for special equipment or supplies, potential referrals to health agencies, and any additional comments that could impact the care plan. This structured approach ensures that all aspects of the patient's health and home care needs are meticulously addressed, facilitating the provision of adequate care and support within the comfort of the patient's home.
| Question | Answer |
|---|---|
| Form Name | Hcsp M11 Q Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | m11q new york, m11q form, emblem m11q form, emblem health 11q form |