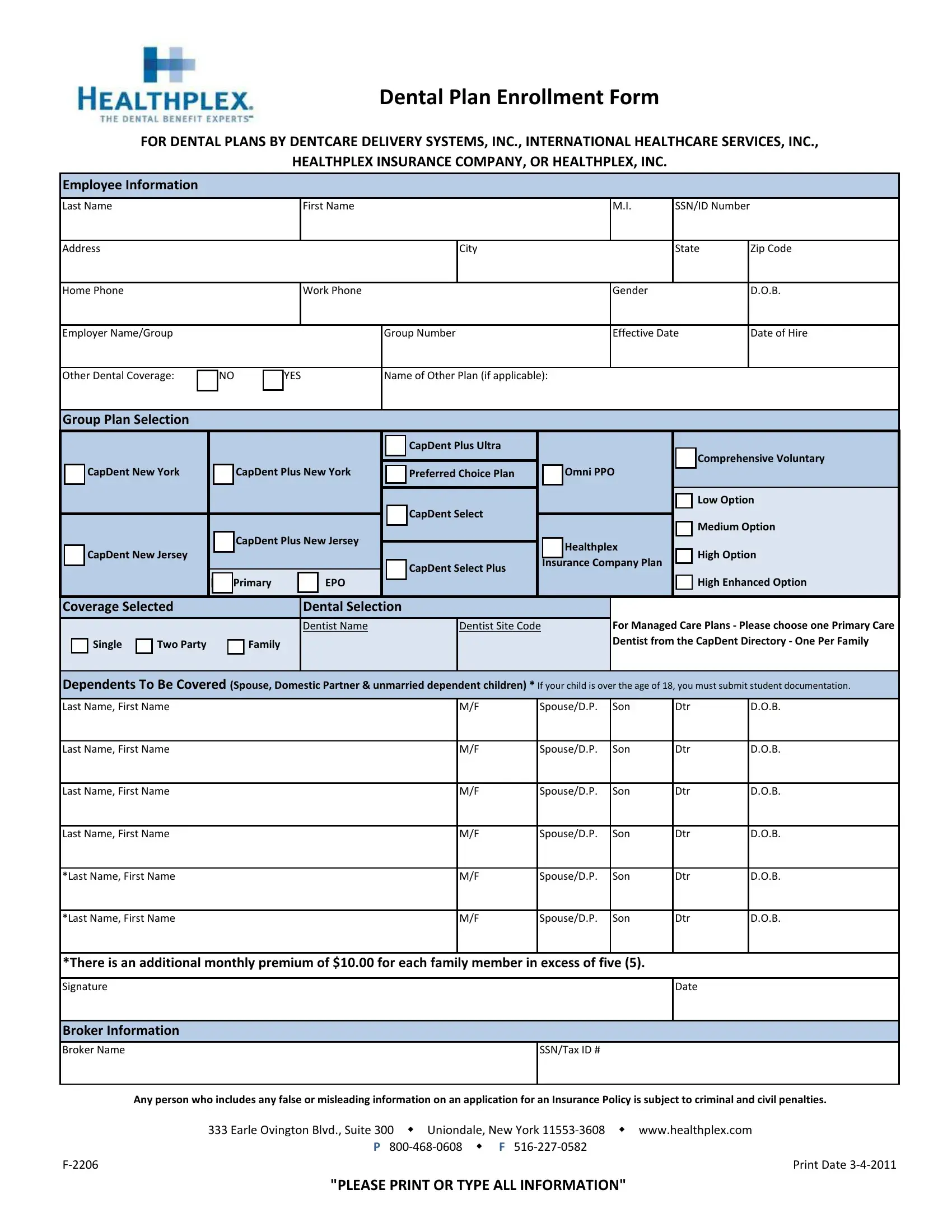
Navigating the complex world of dental insurance enrollment can be a daunting task, but understanding the Healthplex Enrollment Form is a significant first step in gaining access to dental care coverage. This form serves as a gateway for individuals seeking dental insurance through DENTCARE Delivery Systems, Inc., International Healthcare Services, Inc., Healthplex Insurance Company, or Healthplex, Inc. The process begins with personal details, requiring the employee's name, identification, and contact information, followed by employment and insurance details that include the employer's name, group number, and any existing dental coverage. Importantly, the form also delves into the selection of dental plans, offering a range of options from CapDent Plus Ultra to High Enhanced Option, catering to diverse needs and preferences. Each plan is designed to cover individual employees, two-party enrollments, or families, with specific attention to dependents, where it's crucial to note any over the age of 18 may require additional documentation. Unique to managed care plans, enrollees must select a primary care family dentist from a specified directory, emphasizing the focus on personalized dental care. Broker information and a declaration against false information underpin the form's completion, binding the enrollee to honesty and accuracy. Located in Uniondale, New York, Healthplex makes this vital form accessible through their website, simplifying the process of enrolling in comprehensive dental care coverage.
| Question | Answer |
|---|---|
| Form Name | Healthplex Enrollment Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | enrollment healthplex dental, member activate, enrollment forms, healthplex enrollment online |