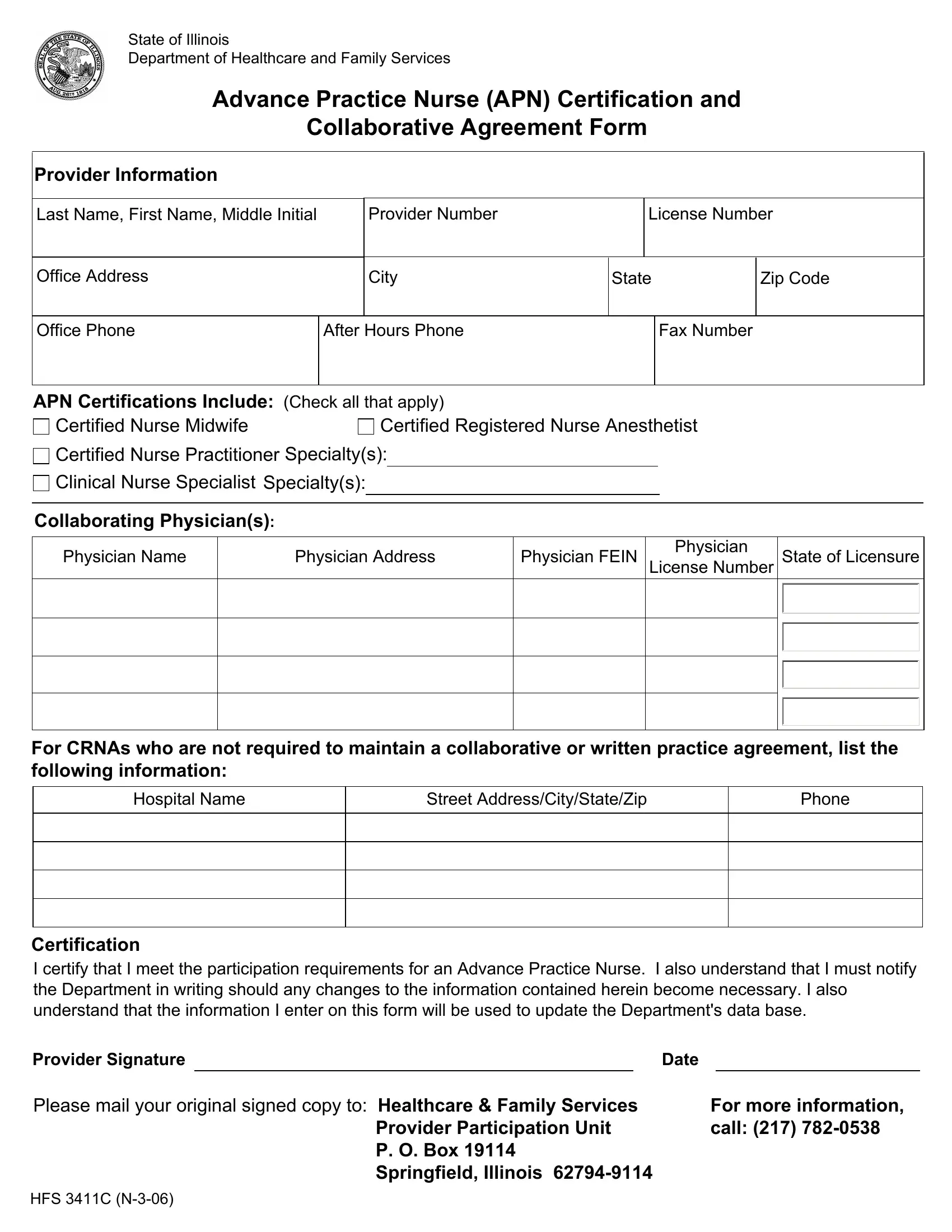
The HFS 3411C form serves a crucial function within the healthcare framework of the State of Illinois, specifically tailored for Advance Practice Nurses (APNs). This form is designed by the Department of Healthcare and Family Services and encompasses a comprehensive set of information that APNs must provide. This includes personal and professional details such as name, contact information, license number, and provider number. Moreover, it encompasses critical areas of specialization, highlighting the diverse roles APNs can hold, including Certified Nurse Midwives, Certified Registered Nurse Anesthetists, Certified Nurse Practitioners, and Clinical Nurse Specialists. Each category allows specification of further specialties, exemplifying the form's role in cataloging the varied expertise within the nursing field. In addition to certifying their qualifications, APNs are required to detail collaborative agreements with physicians, unless exempt, as in the case for some Certified Registered Nurse Anesthetists. Such collaborations are an integral part of nursing practice, ensuring comprehensive patient care through interdisciplinary teamwork. The form also includes a certification statement that underscores the APN's commitment to maintaining the accuracy of their professional information and understanding the obligation to update the Department with any changes. With a clear directive for submission and contact information for further assistance, the HFS 3411C form underscores the structured and regulated environment within which APNs operate, ensuring that their practice is not only certified but also integrated within the broader healthcare system of Illinois.
| Question | Answer |
|---|---|
| Form Name | Hfs 3411C Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | hfs3411c hfs 3411c n 3 06 form |
State of Illinois
Department of Healthcare and Family Services
Advance Practice Nurse (APN) Certification and
Collaborative Agreement Form
Provider Information
Last Name, First Name, Middle Initial
Office Address
Provider Number |
|
License Number |
|
|
|
|
|
City |
State |
Zip Code |
|
|
|
|
|
Office Phone
After Hours Phone
Fax Number
APN Certifications Include: (Check all that apply)
Certified Nurse Midwife |
Certified Registered Nurse Anesthetist |
Certified Nurse Practitioner Specialty(s):
Clinical Nurse Specialist Specialty(s):
Collaborating Physician(s):
Physician Name
Physician Address
Physician FEIN
Physician
License Number
State of Licensure
For CRNAs who are not required to maintain a collaborative or written practice agreement, list the following information:
Hospital Name
Street Address/City/State/Zip
Phone
Certification
I certify that I meet the participation requirements for an Advance Practice Nurse. I also understand that I must notify the Department in writing should any changes to the information contained herein become necessary. I also understand that the information I enter on this form will be used to update the Department's data base.
Provider Signature |
|
|
Date |
|
Please mail your original signed copy to: Healthcare & Family Services |
For more information, |
|||
|
Provider Participation Unit |
call: (217) |
||
|
P. O. Box 19114 |
|
|
|
|
Springfield, Illinois |
|
|
|
HFS 3411C