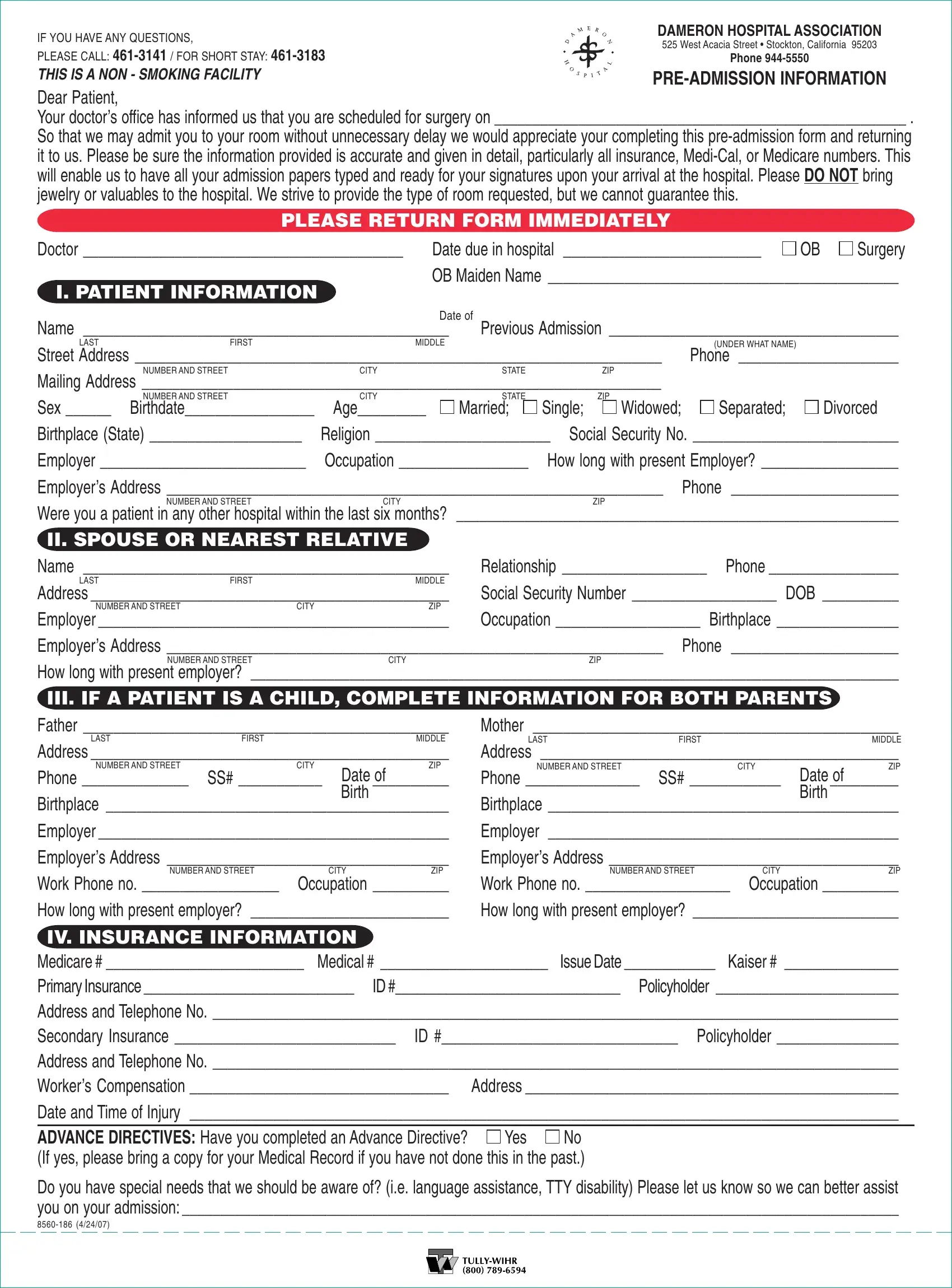
The journey through hospital admission is guided significantly by filling out the Hospital Admission form, an essential step for patients scheduled for surgery or any medical procedure. Dameron Hospital Association, located at 525 West Acacia Street in Stockton, California, emphasizes the importance of providing complete and accurate personal and medical information through the form to ensure a smooth admission process. This comprehensive form covers personal data, including basic identification details, insurance information, and specifics about the patient’s condition and medical history. It also highlights the necessity of avoiding bringing valuables to the non-smoking facility and acknowledges room requests cannot always be guaranteed. Additionally, it carries sections dedicated to spouse or nearest relative information, details relevant if the patient is a child, and crucial insurance data, encompassing Medicare, Medi-Cal, and private insurance specifics. This form also queries about Advance Directives and special needs like language assistance, reinforcing the hospital's commitment to personalized and attentive care from the moment of admission. It stands as a critical document that bridges patients' preparatory process with the hospital's administrative and healthcare delivery systems, designed to streamline the admission process and ensure a focus on health and recovery.
| Question | Answer |
|---|---|
| Form Name | Hospital Admission Form |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 48 |
| Avg. time to fill out | 9 min 51 sec |
| Other names | memorandum of transfer form, hospital memorandum of transfer requirements, hospital memorandum of transfer form, psychiatric hospital admission consent form |
IF YOU HAVE ANY QUESTIONS, |
DAMERON HOSPITAL ASSOCIATION |
|
525 West Acacia Street • Stockton, California 95203 |
||
PLEASE CALL: |
||
PHONE |
||
THIS IS A NON - SMOKING FACILITY |
||
|
||
Dear Patient, |
|
Your doctor’s office has informed us that you are scheduled for surgery on ______________________________________________________ .
So that we may admit you to your room without unnecessary delay we would appreciate your completing this
|
PLEASE RETURN FORM IMMEDIATELY |
|
|
|
||||||
Doctor __________________________________________ |
Date due in hospital |
__________________________ |
OB |
Surgery |
||||||
I. PATIENT INFORMATION |
|
OB Maiden Name ______________________________________________ |
||||||||
|
|
|
|
|
|
|
|
|
||
|
|
|
Date of |
|
|
|
|
|
|
|
Name ________________________________________________ |
Previous Admission ______________________________________ |
|||||||||
LAST |
FIRST |
MIDDLE |
|
|
|
|
(UNDER WHAT NAME) |
|
|
|
Street Address _____________________________________________________________________ |
Phone _____________________ |
|||||||||
|
NUMBER AND STREET |
CITY |
|
STATE |
|
|
ZIP |
|
|
|
Mailing Address ____________________________________________________________________ |
|
|
|
|||||||
|
NUMBER AND STREET |
CITY |
|
STATE |
|
|
ZIP |
|
|
|
Sex ______ |
Birthdate_________________ |
Age_________ |
|
Married; |
Single; |
Widowed; |
Separated; |
|
Divorced |
|
Birthplace (State) ____________________ |
Religion _______________________ |
Social Security No. ___________________________ |
||||||||
Employer ___________________________ |
Occupation _________________ |
How long with present Employer? __________________ |
||||||||
Employer’s Address _________________________________________________________________ Phone ______________________
NUMBER AND STREET |
CITY |
ZIP |
Were you a patient in any other hospital within the last six months? __________________________________________________________
II. SPOUSE OR NEAREST RELATIVE |
|
|
|
||
Name ________________________________________________ |
Relationship ___________________ |
Phone _________________ |
|||
LAST |
FIRST |
|
MIDDLE |
|
|
Address _______________________________________________ |
Social Security Number ___________________ DOB __________ |
||||
NUMBER AND STREET |
CITY |
ZIP |
|
|
|
Employer ______________________________________________ |
Occupation ___________________ Birthplace ________________ |
||||
Employer’s Address _________________________________________________________________ Phone |
______________________ |
||||
|
NUMBER AND STREET |
CITY |
|
ZIP |
|
How long with present employer? _____________________________________________________________________________________
III. IF A PATIENT IS A CHILD, COMPLETE INFORMATION FOR BOTH PARENTS |
|
||||||||
Father ________________________________________________ |
Mother ________________________________________________ |
||||||||
LAST |
FIRST |
|
|
MIDDLE |
LAST |
FIRST |
|
|
MIDDLE |
Address _______________________________________________ |
Address _______________________________________________ |
||||||||
NUMBER AND STREET |
|
CITY |
Date of |
ZIP |
NUMBER AND STREET |
CITY |
Date of |
ZIP |
|
Phone ______________ |
SS# ___________ |
|
Phone _______________ SS# ____________ |
|
|||||
|
|
|
Birth |
|
|
|
|
Birth |
|
Birthplace _____________________________________________ |
Birthplace ______________________________________________ |
||||||||
Employer ______________________________________________ |
Employer |
______________________________________________ |
|||||||
Employer’s Address _____________________________________ |
Employer’s Address ______________________________________ |
||||||||
NUMBER AND STREET |
|
CITY |
ZIP |
|
NUMBER AND STREET |
CITY |
|
ZIP |
|
Work Phone no. __________________ |
Occupation __________ |
Work Phone no. ___________________ Occupation __________ |
|||||||
How long with present employer? __________________________ |
How long with present employer? ___________________________ |
||||||||
IV. INSURANCE INFORMATION |
|
|
|
|
|
|
|||
Medicare # __________________________ Medical # ______________________ |
Issue Date ____________ |
Kaiser # _______________ |
|||||||
Primary Insurance _____________________________ ID #_______________________________ Policyholder ________________________
Address and Telephone No. __________________________________________________________________________________________
Secondary Insurance _____________________________ ID #_______________________________ Policyholder ________________
Address and Telephone No. __________________________________________________________________________________________
Worker’s Compensation __________________________________ Address _________________________________________________
Date and Time of Injury _____________________________________________________________________________________________
ADVANCE DIRECTIVES: Have you completed an Advance Directive? |
Yes |
No |
(If yes, please bring a copy for your Medical Record if you have not done this in the past.)
Do you have special needs that we should be aware of? (i.e. language assistance, TTY disability) Please let us know so we can better assist you on your admission: ______________________________________________________________________________________________